Difference between revisions of "Autopsy"
(→External exam: +link) |
m (→Sample clinical history: make future) |
||
| (148 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
'''Autopsy''' | [[Image:Rembrandt Harmensz. van Rijn 007.jpg|thumb|300px|An autopsy.]] | ||
'''Autopsy''' was once a mainstay of [[pathology]]. It is now in decline and uncommonly done. Fetal autopsy is dealt with in a separate article called ''[[fetal autopsy]]''. | |||
== | =Value of autopsy= | ||
A significant number of major findings cannot be diagnosed without histology;<ref name=pmid16324191>{{Cite journal | last1 = Roulson | first1 = J. | last2 = Benbow | first2 = EW. | last3 = Hasleton | first3 = PS. | title = Discrepancies between clinical and autopsy diagnosis and the value of post mortem histology; a meta-analysis and review. | journal = Histopathology | volume = 47 | issue = 6 | pages = 551-9 | month = Dec | year = 2005 | doi = 10.1111/j.1365-2559.2005.02243.x | PMID = 16324191 }}</ref> thus, without a biopsy or an autopsy they cannot be diagnosed. Autopsies can be regarded as a form of [[quality control]]. | |||
One large review in ''JAMA'' suggests that approximately:<ref name=pmid12783916>{{cite journal |author=Brian Gallagher, Burton EC, McDonald KM, Goldman L |title=Changes in rates of autopsy-detected diagnostic errors over time: a systematic review |journal=JAMA |volume=289 |issue=21 |pages=2849–56 |year=2003 |pmid=12783916 |doi=10.1001/jama.289.21.2849}}</ref> | |||
* 25% of autopsies reveal a finding that would have changed clinical management. | |||
* 5% of autopsies reveal a missed [[diagnosis]] that probably affected the outcome. | |||
== | =Autopsy checklist= | ||
===Minimum to proceed - hospital autopsy=== | |||
*Death certificate complete. | |||
**Cause of death as per death certificate. | |||
*[[Autopsy consent]] properly done. | |||
*Patient identified. | |||
==Spleen== | ===Clinical history checklist - hospital admission=== | ||
*Admit date. | |||
*Admit diagnosis. | |||
**History of illness prior to admission? | |||
*Past medical history. | |||
**Recent hospital admissions? | |||
**Significant medical conditions. | |||
*State preceding death - especially the last 24 hours. | |||
**Level of consciousness. | |||
**Vitals. | |||
*Location at time of death and preceding 24 hours. | |||
**Ward. | |||
**Intensive care unit. | |||
**Other. | |||
*Time immediately prior to death. | |||
**Code called. | |||
**Found cold. | |||
**Other. | |||
*Date and time of death. | |||
*Clinical status prior to death. | |||
**Expected versus unexpected. | |||
=Autopsy consent= | |||
===General=== | |||
*In a hospital autopsy the ''most important'' thing is: ''proper consent''. | |||
*Generally, corner's cases/medical examiner's cases do not require a consent for autopsy; however, the retention of tissue may require consent. | |||
===Who has authority?=== | |||
*Consent should be given by the ''executor of the estate''.<ref name=olduhnconsent>URL: [http://www.docstoc.com/docs/51609856/CONSENT-FOR-AUTOPSY http://www.docstoc.com/docs/51609856/CONSENT-FOR-AUTOPSY]. Accessed on: 27 September 2010.</ref> | |||
====Hierarchy==== | |||
If the ''executor of the estate'' is not specified the hierarchy is as follows:<ref name=olduhnconsent/> | |||
#Spouse - by marriage (same sex ''or'' opposite sex) ''or'' by common-law ''or'' by together the parents of a child ''or'' by cohabitation agreement (in law). | |||
#If no spouse, any children 16+ years old, | |||
#If no children, either parent, | |||
#If no parent, any brother or sister 16+ years old, | |||
#If no sibling, any next-of-kin 16+ years old, | |||
#If no next-of-kin, the person lawfully in possession of the body (''not'' the hospital). | |||
Notes: | |||
*Exact hierarchy may vary by jurisdiction. | |||
*The power a person that is designated as ''power of attorney for health care decisions'' does not have the authority to consent for an autopsy; their power ends with death (unless they are also the ''executor of the estate''). | |||
*In clinical medicine, it is allowable to skip down the hierarchy if ''the'' "consent giver" is not reachable, e.g. if a child of the patient is present they can consent in emergency circumstances, if the spouse is ''not'' reachable. In the context of (non-corner's) autopsies, '''the hierarchy has to be followed strictly''', as there is no such thing as an "emergency autopsy"; it is ''not'' acceptable to ask the child of the decedent 'cause they aren't distraught like the spouse of the decedent. | |||
*In non-corner's cases/non-medical examiner's cases, a physician ''cannot'' give consent for an autopsy. | |||
===Religious objections=== | |||
*There are religious objections to autopsy among Jews and Muslims.<ref name=Ref_HospAuto43>{{Ref HospAuto|43}}</ref><ref name=Ref_HospAuto47>{{Ref HospAuto|47}}</ref> | |||
*It is ''not'' considered good practise to agree to restrictions that will impair a complete assessment, e.g. "stop as soon as one has the cause of death", especially in the medicolegal context (when the extent of the autopsy is at the pathologist's discretion). It is often said that... ''incomplete autopsies give incomplete answers''. | |||
==Timeliness== | |||
There are turnaround time standards from the ''College of American Pathologists'':<ref name=pmid19961247>{{Cite journal | last1 = Siebert | first1 = JR. | title = Increasing the efficiency of autopsy reporting. | journal = Arch Pathol Lab Med | volume = 133 | issue = 12 | pages = 1932-7 | month = Dec | year = 2009 | doi = 10.1043/1543-2165-133.12.1932 | PMID = 19961247 }}</ref> | |||
{| class="wikitable sortable" | |||
! Deliverable | |||
! Time | |||
! Comment | |||
|- | |||
| Provisional report | |||
| 2 working days | |||
| gross findings & history | |||
|- | |||
| "Most" final reports | |||
| 30 days | |||
| | |||
|- | |||
| All final reports | |||
| 60 days | |||
| | |||
|- | |||
|} | |||
=External exam= | |||
===General=== | |||
*Very important in the forensic context. | |||
*Medical devices, tubes and lines should be left ''in situ'' to allow the determination of their precise location within the body;<ref name=Ref_HospAuto101>{{Ref HospAuto|101}}</ref> it is very difficult to determine what the location of a line was once it is removed. | |||
===Extremities=== | |||
*Fingers should be identified by name (e.g. ''ring finger''), as some people number the digits 1-4 and consider the thumb separately, while others number 'em 1-5.<ref>TR. 28 September 2010.</ref> | |||
Body should be examined for ''defensive-type wounds'': | |||
*Between the fingers - especially thumb and pointing finger. | |||
*Dorsal aspect of the hand. | |||
*Forearm. | |||
===Findings=== | |||
*External exam findings are found in the ''[[forensic pathology]]'' article. | |||
=Internal exam= | |||
===General=== | |||
*This is usually where the money is in hospital autopsies. | |||
*Like surgeons say... ''you should never cut anything until you're sure what it is''. | |||
===Before the first incision=== | |||
If there is suspicion of [[pneumothorax]] - one the the three following can be done:<ref name=Ref_HospAuto120-1>{{Ref HospAuto|120-1}}</ref> | |||
#Create a "pleural window" (between ribs by removing soft tissue... without entering the pleural cavity). | |||
#Open chest underwater and watch for air bubbles. | |||
#Needle puncture with water filled syringe - where plunger has been removed. | |||
*If there are neck abnormalities or suspicion of pressure on the neck, it is prudent to remove the cranial contents and thoracic contents ''before'' doing the neck dissection.<ref name=HospAuto118>{{Ref HospAuto|118}}</ref> | |||
**If the above does ''not'' apply, i.e. there is no neck injury/suspected neck injury, the [[tongue]] & neck can be taken together with the thorax pluck or organ pluck. | |||
===Incisions=== | |||
*Y-shaped incision (standard): | |||
**Superior "points" of the Y ~ at the deltoid muscle. | |||
**"Confluence of lines" in the Y ~ inferior to the suprasternal notch. | |||
*Neck dissection incisions: | |||
**Deltoid to mastoid process. | |||
====Chest plate==== | |||
*Removed by cutting the ribs - usu. at the rib ends. | |||
*Ribs should be examined for fractures. | |||
*Usually of no interest. | |||
Notes: | |||
*The sternum may have cleft or foramen - as an anatomical variant.<ref name=pmid10803333>{{cite journal |author=Fokin AA |title=Cleft sternum and sternal foramen |journal=Chest Surg. Clin. N. Am. |volume=10 |issue=2 |pages=261–76 |year=2000 |month=May |pmid=10803333 |doi= |url=}}</ref> | |||
*If the decedent has a history of a [[CABG]] removal of the chest plate should be done with care to preserve the grafts. | |||
===Blood clots - ''pre- and post-mortem''=== | |||
{| class="wikitable sortable" | |||
! Feature/time | |||
! Pre-mortem | |||
! Post-mortem | |||
|- | |||
|Shininess | |||
| dull | |||
| shiny | |||
|- | |||
|Adherent to wall | |||
| yes<ref name=Ref_HospAuto>{{Ref HospAuto|156}}</ref> | |||
| no | |||
|- | |||
|Colour | |||
| grey; may have zebraic <br>appearance (lines of Zahn) - <br>red alt. with grey/yellow | |||
| dark purple ''or''<br> bilayered yellow/red | |||
|- | |||
|Pressurized | |||
| yes; "ejects itself" from lumen | |||
| no; needs to be pulled-out | |||
|- | |||
|Consistency <br>-elastic modulus (E)<br>-fracture toughness (K) | |||
| firm (high E)<br> brittle (low K) | |||
| jello (low E)<br> elastic (high K) | |||
|- | |||
|Image - gross | |||
| [http://www.pathguy.com/lectures/waut033.jpg thrombus (pathguy.com)], <br>[http://www.thrombosisadviser.com/en/image.php?image=thrombus-right-atrial-appendage-pathology&category=atherothrombosis thrombus (thrombosisadviser.com)] | |||
| [http://www.meddean.luc.edu/lumen/meded/MEDICINE/PULMONAR/IMAGES/leischne/L3.JPG coronary thrombus (luc.edu)]<ref>URL: [http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/list.htm http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/list.htm]. Accessed on 8 October 2010.</ref> | |||
|- | |||
|Image - micro. | |||
| [http://www.elsevier.es/ficheros/images/255/255v62n10/origen/255v62n10-13142654fig1.jpg pre- & post-mortem (elsevier.es)]<ref>URL: [http://www.elsevier.es/cardio_eng/ctl_servlet?_f=40&ident=13142654 http://www.elsevier.es/cardio_eng/ctl_servlet?_f=40&ident=13142654]. Accessed on: 8 October 2010.</ref> | |||
| [http://eurheartj.oxfordjournals.org/content/early/2010/01/12/eurheartj.ehp557/F3.expansion.html thrombus (oxfordjournals.org)], <br>[http://pathhsw5m54.ucsf.edu/cts/unknown16/thrombi.html thrombi (ucsf.edu)] | |||
|} | |||
Notes: | |||
*Post-mortem thrombi: one (superior) yellow portion (called "chicken fat") and one (dependent) red portion (RBCs); components layer due to gravity. | |||
===Retrieval of the (organ) "pluck"=== | |||
One piece (standard): | |||
*Diaphragm cut: at chest wall. | |||
*Superior cut: through arch vessels. | |||
*Inferior cut: through the common iliac vessels. | |||
*Posterior: | |||
**Thorax: cut paravertebral. | |||
**Abdomen: blunt dissection for kidneys, then paravertebral. | |||
Two pieces (thorax & abdomen): | |||
*May be preferred in a "glued" (fibrosed/post-surgical) abdomen. | |||
*Procedure - similar to ''one piece'' but: | |||
**Cut aorta distal to the left subclavian + detach from thoracic pluck. | |||
**Cut esophagus distal to pharynx + detach from thoracic pluck. | |||
==Neck organ pluck== | |||
===Non-suspicious cases=== | |||
#Trim tissue posterior to horns of the thyroid. | |||
#Cut between thyroid horns & hyoid. | |||
#Cut off base of tongue. | |||
===Suspicious cases=== | |||
*In Canada, it is convention to do ''layered neck dissection''. | |||
**The strap muscles of the neck are lifted of in layers to look for injuries (mostly contusions). | |||
**Strap muscle hematomas may arise in a number of contexts, e.g. they are reported in drowning.<ref>{{Cite journal | last1 = Püschel | first1 = K. | last2 = Schulz | first2 = F. | last3 = Darrmann | first3 = I. | last4 = Tsokos | first4 = M. | title = Macromorphology and histology of intramuscular hemorrhages in cases of drowning. | journal = Int J Legal Med | volume = 112 | issue = 2 | pages = 101-6 | month = | year = 1999 | doi = | PMID = 10048667 }}</ref> | |||
====Hyoid bone==== | |||
*Important in forensic pathology. | |||
*Fracture is seen in manual [[strangulation]]. | |||
*May appear fractured if triticeous cartilage (or triticeal cartilage) is present;<ref name=pmid15075682>{{cite journal |author=Di Nunno N, Lombardo S, Costantinides F, Di Nunno C |title=Anomalies and alterations of the hyoid-larynx complex in forensic radiographic studies |journal=Am J Forensic Med Pathol |volume=25 |issue=1 |pages=14–9 |year=2004 |month=March |pmid=15075682 |doi= |url=}}</ref><ref>URL: [http://faculty.ksu.edu.sa/Prof.Hamam/curses/Jurnals%20Club/225-Triticeous%20cartilage.pdf http://faculty.ksu.edu.sa/Prof.Hamam/curses/Jurnals%20Club/225-Triticeous%20cartilage.pdf]. Accessed on: 10 September 2010.</ref> triticeous cartilage may be confused with a fragment of hyoid bone. | |||
**''Triticeous'' is pronounced ''tri-tish´us''.<ref>URL: [http://medical-dictionary.thefreedictionary.com/triticeous http://medical-dictionary.thefreedictionary.com/triticeous]. Accessed on: 15 September 2010.</ref> | |||
====Larynx injury==== | |||
These are worked-up in great detail in Germany.<ref name=Gazov>Evgenij Gazov. LMU Rechtsmedizin. 8 July 2011. Possibly described more here: [http://www.reference-global.com/doi/abs/10.1515/9783899496079.1027 http://www.reference-global.com/doi/abs/10.1515/9783899496079.1027]</ref> In Canada, the examination, by comparison, is superficial. A detailed examination of the larynx may offer significant information in [[asphyxial deaths]]. | |||
Process: | |||
*Pre-evaluation - if a larynx injury is suspected: | |||
**The larynx should '''not''' be opened. | |||
**Soft tissue should be removed with blunt dissection. | |||
*Evaluation (done with a stereo microscope): | |||
**Tension - splits/tears, bleeding. | |||
**Compression - surrounding tissue no splits/tears. | |||
**Partial fractures - give information about directionality. | |||
Recognized patterns: | |||
*Left horn of thyroid cartilage fracture - choking with left-handed. | |||
*Right horn of thyroid cartilage fracture - choking with right-hand. | |||
*Cricoid cartilage two fractures anteriolateral - choke hold from behind. | |||
==Dissection of thoraco-abdominal pluck== | |||
===Process=== | |||
#Place organ pluck with anterior aspect down. | |||
#Open aorta (posterior aspect - from just distal to subclavian + common iliacs). | |||
#*Probe celiac trunk, SMA, renal arteries, IMA. | |||
#*Open renal arteries. | |||
#Blunt dissection to separate aorta from thorax distal to left subclavian artery. | |||
#Cut through aorta distal to left subclavian artery. | |||
#Separate aorta from pluck. | |||
#Open IVC to diaphragm. | |||
#*Check renal veins. | |||
#Separate IVC. | |||
#Transect [[esophagus]] (~2 cm) distal to inferior margin of the cricoid cartilage. | |||
#Take down esophagus using blunt dissection (to separate from thorax). | |||
#Separate thorax and abdomen - by dissecting through the [[pericardium]]. | |||
===Common finding(s)=== | |||
*Aorta = [[atherosclerosis]]. | |||
===Things to think about=== | |||
*Renal arteries = atherosclerosis (old), [[fibromuscular dysplasia]] (young). | |||
*Renal veins = [[renal cell carcinoma]]. | |||
==Thoracic pluck== | |||
===Heart=== | |||
*Dissection - see ''[[Heart]]'' article. | |||
*Conducting system - see ''[[Heart]]'' article. | |||
===Respiratory system=== | |||
#Open [[trachea]] + bronchus (see ''Note''). | |||
#Examine proximal airway. | |||
#Examine proximal pulmonary arteries. | |||
#*May be done from intralobular fissures.<ref>Ali-Ridha, HN. 8 October 2010.</ref> | |||
#**The large arteries of the right lung is found deep to oblique fissure.<ref name=Ref_HospAuto156>{{Ref HospAuto|156}}</ref> | |||
#Slice lungs - one lobe at a time (easier to cut). | |||
#Squeeze lungs - to test for the presence of pus and [[pulmonary edema|edema]] fluid.<ref name=Ref_HospAuto156>{{Ref HospAuto|156}}</ref> | |||
Note: | |||
*If the lungs are to be inflated the bronchi should be left long. | |||
====Common findings==== | |||
{{Main|Lung}} | |||
*Plural adhesions. | |||
*Plural [[effusions]]. | |||
**Types: ''serous'' (clear), ''serosaginous'' (cloudy), ''serofibrinous'' (clotted/webbed), ''purulent'' (yellow). | |||
*[[Pulmonary edema|Edema]] - fluid comes-out when you squeeze 'em, "heavy" (large mass). | |||
*[[emphysema|Emphysematous change]] (usu. upper lung zone predominant) +/- black pigment (anthracosis). | |||
*Consolidation - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure; often [[pneumonia]]. | |||
*Atelectasis - depressed red areas.<ref>{{Ref AoGP|90}}</ref> | |||
==Abdominal organ pluck== | |||
===Adrenal glands=== | |||
#Place cuts at anatomical location. | |||
#Take section for stock. | |||
====Common findings==== | |||
{{main|Adrenal gland}} | |||
*[[Adrenal cortical adenoma|Cortical adenoma]]s - seen in ~ 2% of autopsies.<ref name=pmid14514341>{{cite journal |author=Barzon L, Sonino N, Fallo F, Palu G, Boscaro M |title=Prevalence and natural history of adrenal incidentalomas |journal=Eur. J. Endocrinol. |volume=149 |issue=4 |pages=273–85 |year=2003 |month=October |pmid=14514341 |doi= |url=}}</ref> | |||
=====Others===== | |||
*Atrophy - typically iatrogenic, may be [[Addison's disease]]. | |||
*[[Adrenal cortical hyperplasia|Hyperplasia]] (bilateral). | |||
*Hemorrhage ([[Waterhouse-Friderichsen syndrome]]). | |||
*[[Metastatic]] cancer, esp. in the context of lung cancer. | |||
*[[Adrenal myelolipoma]]. | |||
===Stomach=== | |||
*Opened along greater curvature. | |||
**Large carcinomas preferentially involve the lesser curvature.<ref name=pmid2550682>{{Cite journal | last1 = Yamagawa | first1 = H. | last2 = Onishi | first2 = T. | title = [A clinicopathological study of early gastric cancers with a diameter larger than five centimeters]. | journal = Gan No Rinsho | volume = 35 | issue = 10 | pages = 1114-8 | month = Sep | year = 1989 | doi = | PMID = 2550682 }}</ref> | |||
*GE junction should not be opened if [[portal hypertension]] is suspected (see: ''esophagus''). | |||
====Findings==== | |||
{{Main|Stomach}} | |||
*Haemorrhage = usu. post-mortem. | |||
*Small ~1 mm pellets ([http://www.gea-pharma.in/GPSIN/cmsresources.nsf/0/0514D214E17B10C0C125749B002640E1/$File/capsule_type.jpg medicinal capsule contents]). | |||
===Esophagus=== | |||
{{Main|Esophagus}} | |||
*Should be everted, if [[portal hypertension]] is suspected, as [[esophageal varices]] are thus more readily demonstrated.<ref name=Ref_HospAuto140>{{Ref HospAuto|140}}</ref> | |||
*#Stomach opened (''without opening GE junction''). | |||
*#String tied to proximal esophagus. | |||
*#Forceps inserted from stomach to grasp tied end and invert [[esophagus]]. | |||
===Omentum=== | |||
{{Main|Omentum}} | |||
*It is a good idea to trim this from the stomach. | |||
===Spleen=== | |||
#Separate stomach from spleen. | |||
#Identify the splenic vessels. | |||
#To separate the spleen from the pluck: | |||
#*Cut across vessels at splenic hilum - close to the spleen. | |||
====Common findings==== | |||
{{Main|Spleen}} | {{Main|Spleen}} | ||
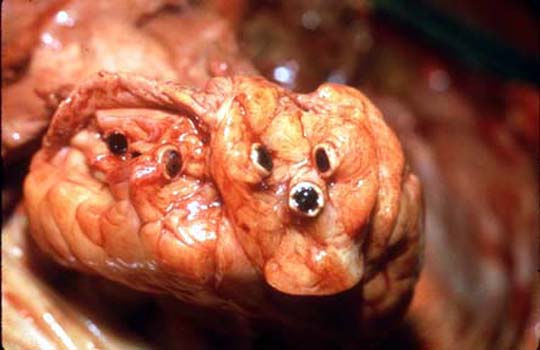
*Sugar-coated spleen. | |||
*Properly referred to as ''hyaloserositis of the spleen''. | **Properly referred to as ''[[hyaloserositis of the spleen]]''. | ||
*Capsule of the spleen is white - resembles sugar-coating. | **Capsule of the spleen is white - resembles sugar-coating. | ||
*Importance: ''none'' - benign. | **Importance: ''none'' - benign. | ||
*[[Splenomegaly]] secondary to [[portal hypertension]]. | |||
== | ===Kidney=== | ||
* | *Renal vein & artery already examined. | ||
#+/-Open ureter. | |||
#Strip capsule. | |||
#'''L'''eft ureter is left '''l'''ong - to tell apart the kidneys. | |||
#Kidney (nearly) bisected in coronal plane from anti-ureteric surface; a small rim of tissue is left on the hilar (or ureteric) aspect -- to keep the kidney as one piece.<ref name=Ref_HospAuto138>{{Ref HospAuto|138}}</ref> | |||
== | ====Common pathologic findings==== | ||
Size of the kidney - small kidneys are seen in chronic renal failure. | *Size of the kidney - small kidneys are seen in chronic renal failure. | ||
**Normal adult kidney ~11 cm from pole-to-pole.<ref name=pmid20030823>{{Cite journal | last1 = Glodny | first1 = B. | last2 = Unterholzner | first2 = V. | last3 = Taferner | first3 = B. | last4 = Hofmann | first4 = KJ. | last5 = Rehder | first5 = P. | last6 = Strasak | first6 = A. | last7 = Petersen | first7 = J. | title = Normal kidney size and its influencing factors - a 64-slice MDCT study of 1.040 asymptomatic patients. | journal = BMC Urol | volume = 9 | issue = | pages = 19 | month = | year = 2009 | doi = 10.1186/1471-2490-9-19 | PMID = 20030823 | URL = http://www.biomedcentral.com/1471-2490/9/19 }}</ref> | |||
*Nephrosclerosis: | |||
**''Flea-bitten appearance'' - seen in [[hypertension]].<ref name=pmid9356598>{{Cite journal | last1 = Ono | first1 = H. | last2 = Ono | first2 = Y. | title = Nephrosclerosis and hypertension. | journal = Med Clin North Am | volume = 81 | issue = 6 | pages = 1273-88 | month = Nov | year = 1997 | doi = | PMID = 9356598 }}</ref> | |||
*[[Acute tubular necrosis]] (ATN). | |||
**ATN is difficult to prove on autopsy material. | |||
**On microscopy, look for:<ref name=pmid19207286>{{Cite journal | last1 = Kocovski | first1 = L. | last2 = Duflou | first2 = J. | title = Can renal acute tubular necrosis be differentiated from autolysis at autopsy? | journal = J Forensic Sci | volume = 54 | issue = 2 | pages = 439-42 | month = Mar | year = 2009 | doi = 10.1111/j.1556-4029.2008.00956.x | PMID = 19207286 }}</ref> | |||
***Tubular epithelial whorls. | |||
***Tubulorrhexis. | |||
***Interstitial edema. | |||
=== | ===Liver=== | ||
#Remove diaphragm (with scissors). | |||
#Separated liver from abdominal pluck at ''porta hepatis''. | |||
#Open [[Gallbladder]]. | |||
#Get mass, i.e. weigh. | |||
#Slice axially - as seen on CT imaging. | |||
Notes: | |||
* | *If there is a suspected biliary tract obstruction: | ||
*#Open the [[duodenum]] (from distal end) and identify the ''duodenal papilla'' - this is usually obvious as everything distal to the duodenal papilla is usually light brown (bile-stained). | |||
* | *#Compress the gallbladder and bile should emerge from the duodenal papilla. | ||
** | *#Disect bilary tree from duodenal papilla to the porta hepatis. | ||
== | ====Common pathologic findings==== | ||
*One should saw through the skull completely, i.e. one should not crack the skull open with a chisel. | =====Liver===== | ||
{{Main|Liver}} | |||
*Firm - suggests [[cirrhosis]]. | |||
*Micronodularity (with uniformity of the nodules) - suggestive of alcoholic cirrhosis. | |||
*Macronodularity (with heterogeneity of the nodules) - suggestive of [[viral hepatitis]]. | |||
*Yellow ''or'' pale liver: | |||
**DDx: | |||
**#Shock liver. | |||
**#[[Liver steatosis|Steatosis]] ''or'' [[steatohepatitis]]. | |||
*Congested (blood red/yellow) "nutmeg liver". | |||
**Image: [http://www.pathology-india.com/nutmegliv1.JPG Nutmeg liver (pathology-india.com)]. | |||
=====Gallbladder===== | |||
{{Main|Gallbladder}} | |||
*Gallstones ([[cholelithiasis]]). | |||
*Mucosa with strawberry-like appearance ([[cholesterolosis of the gallbladder|cholesterolosis]]). | |||
===Pancreas=== | |||
*Serially section along axis of pancreatic duct. | |||
*Pieces of head & tail for stock ''or'' stock and histology. | |||
==Genitourinary-rectal ''or'' pelvic pluck== | |||
===Female<ref name=Ref_HospAuto130>{{Ref HospAuto|130}}</ref>=== | |||
#Orient rectum down, bladder up. | |||
#Open bladder with scissors via urethra with cuts in sagittal plane. | |||
#Flip over specimen. | |||
#Open rectum with scissors with cuts in the sagittal plane. | |||
#Flip over specimen. | |||
#Open vagina with cuts on its lateral aspect. | |||
#Open cervix & uterus with cuts on its lateral aspect. | |||
#Bisect ovaries. | |||
====Common pathologic findings==== | |||
{{Main|Ovary}} | |||
*Ovary: | |||
**Corpus luteum - bright yellow (non-pathologic). | |||
**Simple cyst. | |||
{{Main|Uterus}} | |||
*Uterus: | |||
**Leiomyoma (uterine fibroid). | |||
{{Main|Urinary bladder}} | |||
*Urinary bladder: | |||
**Focal haemorrhage secondary to urinary catheter. | |||
===Male=== | |||
#Orient rectum down, bladder up. | |||
#Open bladder with scissors via urethra/prostate with cuts in sagittal plane. | |||
#Serially section prostate in the planes defined by the axis of the urethra. | |||
#Flip over specimen. | |||
#Open rectum with scissors with cuts in the sagittal plane. | |||
====Common pathologic findings==== | |||
{{Main|Prostate gland}} | |||
*Prostate gland: | |||
**Enlargement ([[benign prostatic hyperplasia]]). | |||
{{Main|Urinary bladder}} | |||
*Urinary bladder: | |||
**Trabeculation secondary to [[BPH]]. | |||
**Focal haemorrhage secondary to urinary catheter. | |||
==Skull & brain== | |||
===Opening the skull=== | |||
#One should saw through the skull completely, i.e. one should not "crack" the skull open with a chisel. | |||
#*Cracking open the skull may result in artefactual fractures that are impossible to differentiate from antemortem fractures. | |||
#*Cuts into the brain from opening the skull ("city morgue sulcus") are ''not'' difficult to distinguish from antemortem injuries. | |||
===Extraction of the brain=== | |||
#Cranial nerves should be cut. | |||
#Tentorium should be released. | |||
#Spinal cord should be completely cut as far down as possible. | |||
#Dura should be stripped from the skull base (to look for [[bone fractures|fractures]]). | |||
Notes: | |||
*[[Scalp hematoma]]: | |||
**May result from intracranial pressure. | |||
***[http://en.wikipedia.org/wiki/File:Scalp_hematomas.jpg Types of scalp hematomas]. | |||
===Brain=== | |||
Considerations for the retension of the brain (for prolonged [[fixation]]): | |||
*Survival interval in hospital. | |||
*Neurosurgical intervention. | |||
*Clinical Dx of [[DAI]]. | |||
*Hypoxic changes (make brain hard to cut). | |||
====Sectioning==== | |||
Up-down anatomically oriented (right side-up): | |||
#Examine meninges. | |||
#Remove dura. | |||
#Examine venous sinuses. | |||
#Look for gyri effacement - due to edema or haematomas. | |||
Not up-down anatomically oriented (top down): | |||
#Remove brain stem - with one cut ~ at level of mid-brain. | |||
#Cerebrum section - first cut at mammillary bodies. | |||
#*Subsequent cuts ~ 1.0 cm in thickness. | |||
===Anatomic variants=== | |||
*Metopic suture - midline in frontal bone.<ref name=pmid19060688>{{cite journal |author=Ramos GA, Ylagan MV, Romine LE, D'Agostini DA, Pretorius DH |title=Diagnostic evaluation of the fetal face using 3-dimensional ultrasound |journal=Ultrasound Q |volume=24 |issue=4 |pages=215–23 |year=2008 |month=December |pmid=19060688 |doi=10.1097/RUQ.0b013e31819073c2 |url=}}</ref> | |||
*Wormian bones = "extra" bone at the sutures in the skull. | |||
===Anatomy=== | |||
*Lambdoidal suture - occipital bone/parietal bones. | |||
*Coronal suture - frontal bone/parietal bone. | |||
==Weird stuff== | ==Weird stuff== | ||
| Line 43: | Line 465: | ||
*Hyperviscosity syndrome - in leukemia.<Ref>[http://cat.inist.fr/?aModele=afficheN&cpsidt=18942659 http://cat.inist.fr/?aModele=afficheN&cpsidt=18942659]</ref> | *Hyperviscosity syndrome - in leukemia.<Ref>[http://cat.inist.fr/?aModele=afficheN&cpsidt=18942659 http://cat.inist.fr/?aModele=afficheN&cpsidt=18942659]</ref> | ||
== | ===Starvation=== | ||
*Normal organ | {{Main|Starvation}} | ||
*Serous fat atrophy. | |||
**Gross appearance: brown goo replaces fat. | |||
***May be associated with blood vessel tortuosity.<ref>KC. 14 September 2010.</ref> | |||
=Histology= | |||
===General=== | |||
It's the at the pathologists discretion. In ''[[decomp]]'' cases it is reasonable to submit nothing. | |||
===Forensic context=== | |||
A standard (minimum) for adult homicides is: | |||
#[[Heart]] (1). | |||
#[[Lung]] (1). | |||
#[[Liver]] (1). | |||
#[[Kidney]] (1). | |||
===Hospital autopsies=== | |||
====Non-neuropathology==== | |||
A standard based on a Toronto teaching hospital: | |||
*[[Thyroid gland]] (1). | |||
*[[Lung]] - each lobe (5). | |||
*[[Heart]] - posterior papillary muscle & LV, anterior papillary muscle & LV (2). | |||
**More extensive histologic sectioning is discussed in the ''[[heart]]'' article. | |||
*[[Liver]] - left lobe, right lobe (2). | |||
*[[Spleen]] - including hilum & capsule (1). | |||
*[[Adrenal gland]] (1). | |||
*Gastrointestinal tract: | |||
**The quality is often very poor (even in "fresh" bodies). These are often omitted. | |||
***[[Pancreas]] - head & tail (1). | |||
***[[Stomach]] (1). | |||
***[[Esophagus]] (1). | |||
***[[Small bowel]] (1). | |||
***Large bowel (1). | |||
*Genitourinary tract: | |||
**[[Kidney]] - each side (2). | |||
**Gender specific: | |||
***Male: | |||
****[[Prostate gland]] (1). | |||
****[[Testis]] (1). | |||
***Female: | |||
****[[Uterus]] +/- cervix (1). | |||
****[[Ovary]] + tube (1). | |||
*[[Bone marrow]] (1). | |||
====Neuro==== | |||
*[[Pituitary gland]] (1). | |||
*Cortex usu. frontal/parietal (1). | |||
*[[Hippocampus]] (1). | |||
*Cerebellum (1). | |||
*Brain stem (1). | |||
*Basal ganglia (1). | |||
====Stock==== | |||
*Thyroid gland. | |||
*Heart: | |||
**Complete (axial) slice (including RV and LV). | |||
**Tissue with SA node. | |||
**Tissue with AV node. | |||
*Lung - all five lobes. | |||
*[[Spleen]]. | |||
*Urinary: | |||
**Kidney. | |||
**Urinary bladder. | |||
*Gastrointestinal tract: | |||
**GE junction. | |||
**Stomach. | |||
**Small bowel. | |||
**Large bowel. | |||
**[[Appendix]]. | |||
**[[Pancreas]] (head & tail). | |||
**Liver. | |||
*Reproductive: | |||
**Male: | |||
***[[Prostate gland]]. | |||
***[[Testis]]. | |||
**Female: | |||
***[[Breast]]. | |||
***[[Uterus]]. | |||
***[[Ovary]]. | |||
*Neurologic: | |||
**Hippocampus + basal ganglia. | |||
**Cortex. | |||
**Brainstem. | |||
**Cerebellum. | |||
*Skin. | |||
*Nerve. | |||
*Muscle. | |||
*[[Lymph nodes]]. | |||
=Autopsy report= | |||
==Normal size parameters== | |||
===Normal organ masses (adult)=== | |||
Caucasoid population of 684 adults:<ref name=pmid11376980>{{cite journal |author=de la Grandmaison GL, Clairand I, Durigon M |title=Organ weight in 684 adult autopsies: new tables for a Caucasoid population |journal=Forensic Sci. Int. |volume=119 |issue=2 |pages=149–54 |year=2001 |month=June |pmid=11376980 |doi= |url=}}</ref> | |||
{| class="wikitable" | |||
| | |||
|'''Men''' | |||
|'''Women''' | |||
|- | |||
|'''Heart''' | |||
|365 +/- 71 g | |||
|312 +/- 78 g | |||
|- | |||
|'''Right lung''' | |||
|663 +/- 239 g | |||
|546 +/- 207 g | |||
|- | |||
|'''Left lung''' | |||
|583 +/- 216 g | |||
|467 +/- 174 g | |||
|- | |||
|'''Liver''' | |||
|1677 +/- 396 g | |||
|1475 +/- 362 g | |||
|- | |||
|'''Spleen''' | |||
|156 +/- 87 g | |||
|140 +/- 78 g | |||
|- | |||
|'''Right kidney''' | |||
|162 +/- 39 g | |||
|135 +/- 39 g | |||
|- | |||
|'''Left kidney''' | |||
|160 +/- 41 g | |||
|136 +/- 37 g | |||
|} | |||
===Pediatrics=== | |||
{{Main|Growth charts}} | |||
==Negative autopsy== | |||
Definition: | |||
*A ''negative autopsy'' is a post-mortem exam that has no anatomical or toxicological cause of death. | |||
**This does ''not'' preclude the presence of pathology (that is not sufficient to cause death). | |||
Cause of death (in a negative autopsy): | |||
*Unascertained. | |||
===Considerations=== | |||
*[[Channelopathy]] - may be elucidated by molecular testing. | |||
*[[Electrocution]] (unrecognized). | |||
*Decomposition. | |||
*Sudden Unexpected Death in [[Epilepsy]] ([[SUDEP]])<ref>URL: [http://emedicine.medscape.com/article/1187111-overview http://emedicine.medscape.com/article/1187111-overview]. Accessed on: 11 October 2010.</ref> - missing history. | |||
*[[Sudden infant death syndrome]]. | |||
==Histology checklist== | |||
{| class="wikitable sortable" | |||
! Section/organ | |||
! Expected finding(s)/common finding(s) | |||
! Findings to consider | |||
|- | |||
| [[Bone marrow]] | |||
| | |||
*trilineage hematopoiesis | |||
| | |||
*infection | |||
*tumour | |||
|- | |||
| [[Coronary arteries]] | |||
| | |||
*[[atherosclerosis]] - should give percent stenosis for major arteries (LMCA, LAD, LCx, RCA) | |||
| | |||
*atherosclerotic plaque rupture | |||
*thrombi | |||
*inflammation | |||
|- | |||
| [[Heart]] muscle | |||
| | |||
*fibrosis - esp. post. LV (old [[myocardial infarction|MI]]) | |||
*nuclear enlargement, arteriolosclerosis, periarteriolar fibrosis ([[hypertensive heart disease]]) | |||
| | |||
*hemorrhage | |||
*wavy fibres (early ischemic change) | |||
*[[necrosis]] - coagulative/contraction band (recent MI) | |||
*inflammatory infiltrate - not associated with necrosis | |||
*hyaline material ([[cardiac amyloidosis]]) | |||
*fibre disarray ([[hypertrophic cardiomyopathy]]) | |||
*fatty replacement ([[ARVC]]) | |||
|- | |||
| [[Adrenal gland]] | |||
| | |||
*no pathology | |||
| | |||
*tumour | |||
**primary (cortex, medulla) | |||
**metastatic | |||
*hemorrhage | |||
*fat | |||
|- | |||
| [[Kidney]] | |||
| | |||
*vessels (atherosclerosis, [[arterial hyaline|arteriolar hyalinization]]) | |||
| | |||
*tumour | |||
*glomeruli (enlargement, crescents, [[mesangial expansion]], inflammation - esp. [[PMN]]s) | |||
*vessels - thrombi ([[thrombotic microangiopathy]]) | |||
*interstitial (fibrosis, inflammation, edema) | |||
*tubules (inflammation, tubular epithelial whorls, tubulorrhexis) | |||
|- | |||
| [[Liver]] | |||
| | |||
*steatosis - should give severity (mild, mederate, severe), location & type (macrovesicular vs. microvesicular) | |||
| | |||
*fibrosis (septa, rounded contours, [[cirrhosis]]), inflammation (cell type, location (portal, interface, lobular)) | |||
*tumour - esp. metastatic | |||
*bile ducts | |||
*[[ballooning degeneration]] ([[steatohepatitis]])/feathery degeneration ([[cholestasis]]) | |||
*necrosis (location important) | |||
|- | |||
| [[Spleen]] | |||
| | |||
*normal white pulp/red pulp | |||
| | |||
*tumour | |||
*surface abnormalities | |||
|- | |||
| Gastrointestinal tract | |||
| | |||
*autolytic changes | |||
| | |||
*tumour | |||
*vessels | |||
*inflammation - esp. [[PMN]]s | |||
*fibrosis | |||
|- | |||
| [[Thyroid gland]] | |||
| | |||
*no pathology | |||
| | |||
*tumour - papillary thyroid carcinoma, goitre | |||
*inflammation | |||
|- | |||
| [[Lung pathology|Lung]] | |||
| | |||
*pulmonary edema | |||
*[[emphysema]] | |||
| | |||
*infectious pneumonia | |||
*[[pulmonary hypertension]] (may be focal) | |||
*interstitial fibrosis | |||
*tumour | |||
*[[granuloma]]s | |||
*hemorrhage | |||
*hyaline membranes ([[diffuse alveolar damage]]) | |||
|} | |||
===List form=== | |||
====Bone marrow==== | |||
*Trilineage hematopoiesis present. | |||
*Negative for infection and negative for tumour. | |||
====Cardiovascular system==== | |||
[[Coronary arteries]]: | |||
*[[Atherosclerosis]] in the: | |||
**Left main coronary artery. | |||
**Left anterior descending coronary artery. | |||
**Left circumflex coronary artery. | |||
**Right coronary artery. | |||
*No identified atherosclerotic plaque rupture. | |||
*No thrombosis. | |||
*No vasculitis. | |||
[[Heart]] muscle: | |||
*Fibrosis - posterior left ventricle. | |||
*Nuclear enlargement, arteriolosclerosis and periarteriolar fibrosis. | |||
*No hemorrhage. | |||
*No wavy fibres. | |||
*No [[necrosis]]. | |||
*No inflammatory infiltrate. | |||
*No hyaline material. | |||
====Endocrine organs==== | |||
[[Adrenal gland]]: | |||
*No pathology apparent. | |||
*No tumour. | |||
*No hemorrhage. | |||
*No fatty replacement. | |||
Thyroid gland: | |||
*Normal thyroid gland. | |||
*No tumour. | |||
*No inflammation. | |||
====Genitourinary system==== | |||
[[Kidney]]: | |||
*Atherosclerosis, mild. | |||
*Arteriolar hyalinization. | |||
*No tumour. | |||
*Normal glomeruli (no enlargement, no crescents, no [[mesangial expansion]], no inflammation). | |||
*No thrombi. | |||
*No interstitial fibrosis, no inflammation, and no edema. | |||
*No tubular inflammation, no whorls, and no fragmentation. | |||
*No apparently pathologic renal casts. | |||
====Gastrointestinal system==== | |||
[[Liver]] | |||
*Steatosis - mild, centrilobular, macrovesicular. | |||
*No fibrosis. | |||
*No inflammation. | |||
*No tumour. | |||
*Normal bile ducts. | |||
*No [[ballooning degeneration]] and no feathery degeneration. | |||
*No necrosis. | |||
Luminal GI tract: | |||
*Autolytic changes. | |||
*No tumour | |||
*No vasculitis. | |||
*No siginificant atherosclerosis. | |||
*No inflammation. | |||
*No fibrosis. | |||
====Spleen==== | |||
*Normal white pulp/red pulp. | |||
*No tumour. | |||
*No surface abnormalities. | |||
====Lung==== | |||
*Pulmonary edema. | |||
*Infectious pneumonia, mild. | |||
*Emphysema, mild. | |||
*No pulmonary hypertension. | |||
*No interstitial fibrosis. | |||
*No tumour, | |||
*No granulomas, | |||
*No significant hemorrhage. | |||
*No hyaline membranes. | |||
==Sign out== | |||
===Sample clinical history=== | |||
<pre> | |||
A 63 year old male with a history of alcohol abuse was admitted on December 13, 2022 for | |||
recurrent alcohol related pancreatitis. On December 21, he was found unresponsive at 0:15. | |||
Approximately fifteen minutes earlier, he was on oxygen and in no apparent distress. A code | |||
blue was called; however, the attempted resuscitation was unsuccessful. Death was declared | |||
at 1:00 on December 21, 2022. | |||
</pre> | |||
=See also= | |||
*[[Fetal autopsy]]. | *[[Fetal autopsy]]. | ||
*[[Forensic pathology]]. | *[[Forensic pathology]]. | ||
=References= | |||
{{reflist|2}} | {{reflist|2}} | ||
=External links= | |||
[[Category:Autopsy]] | [[Category:Autopsy]] | ||
Latest revision as of 21:28, 25 February 2019

Autopsy was once a mainstay of pathology. It is now in decline and uncommonly done. Fetal autopsy is dealt with in a separate article called fetal autopsy.
Value of autopsy
A significant number of major findings cannot be diagnosed without histology;[1] thus, without a biopsy or an autopsy they cannot be diagnosed. Autopsies can be regarded as a form of quality control.
One large review in JAMA suggests that approximately:[2]
- 25% of autopsies reveal a finding that would have changed clinical management.
- 5% of autopsies reveal a missed diagnosis that probably affected the outcome.
Autopsy checklist
Minimum to proceed - hospital autopsy
- Death certificate complete.
- Cause of death as per death certificate.
- Autopsy consent properly done.
- Patient identified.
Clinical history checklist - hospital admission
- Admit date.
- Admit diagnosis.
- History of illness prior to admission?
- Past medical history.
- Recent hospital admissions?
- Significant medical conditions.
- State preceding death - especially the last 24 hours.
- Level of consciousness.
- Vitals.
- Location at time of death and preceding 24 hours.
- Ward.
- Intensive care unit.
- Other.
- Time immediately prior to death.
- Code called.
- Found cold.
- Other.
- Date and time of death.
- Clinical status prior to death.
- Expected versus unexpected.
Autopsy consent
General
- In a hospital autopsy the most important thing is: proper consent.
- Generally, corner's cases/medical examiner's cases do not require a consent for autopsy; however, the retention of tissue may require consent.
Who has authority?
- Consent should be given by the executor of the estate.[3]
Hierarchy
If the executor of the estate is not specified the hierarchy is as follows:[3]
- Spouse - by marriage (same sex or opposite sex) or by common-law or by together the parents of a child or by cohabitation agreement (in law).
- If no spouse, any children 16+ years old,
- If no children, either parent,
- If no parent, any brother or sister 16+ years old,
- If no sibling, any next-of-kin 16+ years old,
- If no next-of-kin, the person lawfully in possession of the body (not the hospital).
Notes:
- Exact hierarchy may vary by jurisdiction.
- The power a person that is designated as power of attorney for health care decisions does not have the authority to consent for an autopsy; their power ends with death (unless they are also the executor of the estate).
- In clinical medicine, it is allowable to skip down the hierarchy if the "consent giver" is not reachable, e.g. if a child of the patient is present they can consent in emergency circumstances, if the spouse is not reachable. In the context of (non-corner's) autopsies, the hierarchy has to be followed strictly, as there is no such thing as an "emergency autopsy"; it is not acceptable to ask the child of the decedent 'cause they aren't distraught like the spouse of the decedent.
- In non-corner's cases/non-medical examiner's cases, a physician cannot give consent for an autopsy.
Religious objections
- There are religious objections to autopsy among Jews and Muslims.[4][5]
- It is not considered good practise to agree to restrictions that will impair a complete assessment, e.g. "stop as soon as one has the cause of death", especially in the medicolegal context (when the extent of the autopsy is at the pathologist's discretion). It is often said that... incomplete autopsies give incomplete answers.
Timeliness
There are turnaround time standards from the College of American Pathologists:[6]
| Deliverable | Time | Comment |
|---|---|---|
| Provisional report | 2 working days | gross findings & history |
| "Most" final reports | 30 days | |
| All final reports | 60 days |
External exam
General
- Very important in the forensic context.
- Medical devices, tubes and lines should be left in situ to allow the determination of their precise location within the body;[7] it is very difficult to determine what the location of a line was once it is removed.
Extremities
- Fingers should be identified by name (e.g. ring finger), as some people number the digits 1-4 and consider the thumb separately, while others number 'em 1-5.[8]
Body should be examined for defensive-type wounds:
- Between the fingers - especially thumb and pointing finger.
- Dorsal aspect of the hand.
- Forearm.
Findings
- External exam findings are found in the forensic pathology article.
Internal exam
General
- This is usually where the money is in hospital autopsies.
- Like surgeons say... you should never cut anything until you're sure what it is.
Before the first incision
If there is suspicion of pneumothorax - one the the three following can be done:[9]
- Create a "pleural window" (between ribs by removing soft tissue... without entering the pleural cavity).
- Open chest underwater and watch for air bubbles.
- Needle puncture with water filled syringe - where plunger has been removed.
- If there are neck abnormalities or suspicion of pressure on the neck, it is prudent to remove the cranial contents and thoracic contents before doing the neck dissection.[10]
- If the above does not apply, i.e. there is no neck injury/suspected neck injury, the tongue & neck can be taken together with the thorax pluck or organ pluck.
Incisions
- Y-shaped incision (standard):
- Superior "points" of the Y ~ at the deltoid muscle.
- "Confluence of lines" in the Y ~ inferior to the suprasternal notch.
- Neck dissection incisions:
- Deltoid to mastoid process.
Chest plate
- Removed by cutting the ribs - usu. at the rib ends.
- Ribs should be examined for fractures.
- Usually of no interest.
Notes:
- The sternum may have cleft or foramen - as an anatomical variant.[11]
- If the decedent has a history of a CABG removal of the chest plate should be done with care to preserve the grafts.
Blood clots - pre- and post-mortem
| Feature/time | Pre-mortem | Post-mortem |
|---|---|---|
| Shininess | dull | shiny |
| Adherent to wall | yes[12] | no |
| Colour | grey; may have zebraic appearance (lines of Zahn) - red alt. with grey/yellow |
dark purple or bilayered yellow/red |
| Pressurized | yes; "ejects itself" from lumen | no; needs to be pulled-out |
| Consistency -elastic modulus (E) -fracture toughness (K) |
firm (high E) brittle (low K) |
jello (low E) elastic (high K) |
| Image - gross | thrombus (pathguy.com), thrombus (thrombosisadviser.com) |
coronary thrombus (luc.edu)[13] |
| Image - micro. | pre- & post-mortem (elsevier.es)[14] | thrombus (oxfordjournals.org), thrombi (ucsf.edu) |
{kind=link}
{kind=link}
{kind=link}
Notes:
- Post-mortem thrombi: one (superior) yellow portion (called "chicken fat") and one (dependent) red portion (RBCs); components layer due to gravity.
Retrieval of the (organ) "pluck"
One piece (standard):
- Diaphragm cut: at chest wall.
- Superior cut: through arch vessels.
- Inferior cut: through the common iliac vessels.
- Posterior:
- Thorax: cut paravertebral.
- Abdomen: blunt dissection for kidneys, then paravertebral.
Two pieces (thorax & abdomen):
- May be preferred in a "glued" (fibrosed/post-surgical) abdomen.
- Procedure - similar to one piece but:
- Cut aorta distal to the left subclavian + detach from thoracic pluck.
- Cut esophagus distal to pharynx + detach from thoracic pluck.
Neck organ pluck
Non-suspicious cases
- Trim tissue posterior to horns of the thyroid.
- Cut between thyroid horns & hyoid.
- Cut off base of tongue.
Suspicious cases
- In Canada, it is convention to do layered neck dissection.
- The strap muscles of the neck are lifted of in layers to look for injuries (mostly contusions).
- Strap muscle hematomas may arise in a number of contexts, e.g. they are reported in drowning.[15]
Hyoid bone
- Important in forensic pathology.
- Fracture is seen in manual strangulation.
- May appear fractured if triticeous cartilage (or triticeal cartilage) is present;[16][17] triticeous cartilage may be confused with a fragment of hyoid bone.
- Triticeous is pronounced tri-tish´us.[18]
Larynx injury
These are worked-up in great detail in Germany.[19] In Canada, the examination, by comparison, is superficial. A detailed examination of the larynx may offer significant information in asphyxial deaths.
Process:
- Pre-evaluation - if a larynx injury is suspected:
- The larynx should not be opened.
- Soft tissue should be removed with blunt dissection.
- Evaluation (done with a stereo microscope):
- Tension - splits/tears, bleeding.
- Compression - surrounding tissue no splits/tears.
- Partial fractures - give information about directionality.
Recognized patterns:
- Left horn of thyroid cartilage fracture - choking with left-handed.
- Right horn of thyroid cartilage fracture - choking with right-hand.
- Cricoid cartilage two fractures anteriolateral - choke hold from behind.
Dissection of thoraco-abdominal pluck
Process
- Place organ pluck with anterior aspect down.
- Open aorta (posterior aspect - from just distal to subclavian + common iliacs).
- Probe celiac trunk, SMA, renal arteries, IMA.
- Open renal arteries.
- Blunt dissection to separate aorta from thorax distal to left subclavian artery.
- Cut through aorta distal to left subclavian artery.
- Separate aorta from pluck.
- Open IVC to diaphragm.
- Check renal veins.
- Separate IVC.
- Transect esophagus (~2 cm) distal to inferior margin of the cricoid cartilage.
- Take down esophagus using blunt dissection (to separate from thorax).
- Separate thorax and abdomen - by dissecting through the pericardium.
Common finding(s)
- Aorta = atherosclerosis.
Things to think about
- Renal arteries = atherosclerosis (old), fibromuscular dysplasia (young).
- Renal veins = renal cell carcinoma.
Thoracic pluck
Heart
Respiratory system
- Open trachea + bronchus (see Note).
- Examine proximal airway.
- Examine proximal pulmonary arteries.
- Slice lungs - one lobe at a time (easier to cut).
- Squeeze lungs - to test for the presence of pus and edema fluid.[21]
Note:
- If the lungs are to be inflated the bronchi should be left long.
Common findings
- Plural adhesions.
- Plural effusions.
- Types: serous (clear), serosaginous (cloudy), serofibrinous (clotted/webbed), purulent (yellow).
- Edema - fluid comes-out when you squeeze 'em, "heavy" (large mass).
- Emphysematous change (usu. upper lung zone predominant) +/- black pigment (anthracosis).
- Consolidation - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure; often pneumonia.
- Atelectasis - depressed red areas.[22]
Abdominal organ pluck
Adrenal glands
- Place cuts at anatomical location.
- Take section for stock.
Common findings
- Cortical adenomas - seen in ~ 2% of autopsies.[23]
Others
- Atrophy - typically iatrogenic, may be Addison's disease.
- Hyperplasia (bilateral).
- Hemorrhage (Waterhouse-Friderichsen syndrome).
- Metastatic cancer, esp. in the context of lung cancer.
- Adrenal myelolipoma.
Stomach
- Opened along greater curvature.
- Large carcinomas preferentially involve the lesser curvature.[24]
- GE junction should not be opened if portal hypertension is suspected (see: esophagus).
Findings
- Haemorrhage = usu. post-mortem.
- Small ~1 mm pellets (medicinal capsule contents).
{kind=link}
Esophagus
- Should be everted, if portal hypertension is suspected, as esophageal varices are thus more readily demonstrated.[25]
- Stomach opened (without opening GE junction).
- String tied to proximal esophagus.
- Forceps inserted from stomach to grasp tied end and invert esophagus.
Omentum
- It is a good idea to trim this from the stomach.
Spleen
- Separate stomach from spleen.
- Identify the splenic vessels.
- To separate the spleen from the pluck:
- Cut across vessels at splenic hilum - close to the spleen.
Common findings
- Sugar-coated spleen.
- Properly referred to as hyaloserositis of the spleen.
- Capsule of the spleen is white - resembles sugar-coating.
- Importance: none - benign.
- Splenomegaly secondary to portal hypertension.
Kidney
- Renal vein & artery already examined.
- +/-Open ureter.
- Strip capsule.
- Left ureter is left long - to tell apart the kidneys.
- Kidney (nearly) bisected in coronal plane from anti-ureteric surface; a small rim of tissue is left on the hilar (or ureteric) aspect -- to keep the kidney as one piece.[26]
Common pathologic findings
- Size of the kidney - small kidneys are seen in chronic renal failure.
- Normal adult kidney ~11 cm from pole-to-pole.[27]
- Nephrosclerosis:
- Flea-bitten appearance - seen in hypertension.[28]
- Acute tubular necrosis (ATN).
- ATN is difficult to prove on autopsy material.
- On microscopy, look for:[29]
- Tubular epithelial whorls.
- Tubulorrhexis.
- Interstitial edema.
Liver
- Remove diaphragm (with scissors).
- Separated liver from abdominal pluck at porta hepatis.
- Open Gallbladder.
- Get mass, i.e. weigh.
- Slice axially - as seen on CT imaging.
Notes:
- If there is a suspected biliary tract obstruction:
- Open the duodenum (from distal end) and identify the duodenal papilla - this is usually obvious as everything distal to the duodenal papilla is usually light brown (bile-stained).
- Compress the gallbladder and bile should emerge from the duodenal papilla.
- Disect bilary tree from duodenal papilla to the porta hepatis.
Common pathologic findings
Liver
- Firm - suggests cirrhosis.
- Micronodularity (with uniformity of the nodules) - suggestive of alcoholic cirrhosis.
- Macronodularity (with heterogeneity of the nodules) - suggestive of viral hepatitis.
- Yellow or pale liver:
- DDx:
- Shock liver.
- Steatosis or steatohepatitis.
- DDx:
- Congested (blood red/yellow) "nutmeg liver".
{kind=link}
Gallbladder
- Gallstones (cholelithiasis).
- Mucosa with strawberry-like appearance (cholesterolosis).
Pancreas
- Serially section along axis of pancreatic duct.
- Pieces of head & tail for stock or stock and histology.
Genitourinary-rectal or pelvic pluck
Female[30]
- Orient rectum down, bladder up.
- Open bladder with scissors via urethra with cuts in sagittal plane.
- Flip over specimen.
- Open rectum with scissors with cuts in the sagittal plane.
- Flip over specimen.
- Open vagina with cuts on its lateral aspect.
- Open cervix & uterus with cuts on its lateral aspect.
- Bisect ovaries.
Common pathologic findings
- Ovary:
- Corpus luteum - bright yellow (non-pathologic).
- Simple cyst.
- Uterus:
- Leiomyoma (uterine fibroid).
- Urinary bladder:
- Focal haemorrhage secondary to urinary catheter.
Male
- Orient rectum down, bladder up.
- Open bladder with scissors via urethra/prostate with cuts in sagittal plane.
- Serially section prostate in the planes defined by the axis of the urethra.
- Flip over specimen.
- Open rectum with scissors with cuts in the sagittal plane.
Common pathologic findings
- Prostate gland:
- Enlargement (benign prostatic hyperplasia).
- Urinary bladder:
- Trabeculation secondary to BPH.
- Focal haemorrhage secondary to urinary catheter.
Skull & brain
Opening the skull
- One should saw through the skull completely, i.e. one should not "crack" the skull open with a chisel.
- Cracking open the skull may result in artefactual fractures that are impossible to differentiate from antemortem fractures.
- Cuts into the brain from opening the skull ("city morgue sulcus") are not difficult to distinguish from antemortem injuries.
Extraction of the brain
- Cranial nerves should be cut.
- Tentorium should be released.
- Spinal cord should be completely cut as far down as possible.
- Dura should be stripped from the skull base (to look for fractures).
Notes:
- Scalp hematoma:
- May result from intracranial pressure.
{kind=link}
Brain
Considerations for the retension of the brain (for prolonged fixation):
- Survival interval in hospital.
- Neurosurgical intervention.
- Clinical Dx of DAI.
- Hypoxic changes (make brain hard to cut).
Sectioning
Up-down anatomically oriented (right side-up):
- Examine meninges.
- Remove dura.
- Examine venous sinuses.
- Look for gyri effacement - due to edema or haematomas.
Not up-down anatomically oriented (top down):
- Remove brain stem - with one cut ~ at level of mid-brain.
- Cerebrum section - first cut at mammillary bodies.
- Subsequent cuts ~ 1.0 cm in thickness.
Anatomic variants
- Metopic suture - midline in frontal bone.[31]
- Wormian bones = "extra" bone at the sutures in the skull.
Anatomy
- Lambdoidal suture - occipital bone/parietal bones.
- Coronal suture - frontal bone/parietal bone.
Weird stuff
- Leukostasis in acute myelogenous leukemia can lead to congestion of organs and fatal haemorrhages.
- Hyperviscosity syndrome - in leukemia.[34]
Starvation
- Serous fat atrophy.
- Gross appearance: brown goo replaces fat.
- May be associated with blood vessel tortuosity.[35]
- Gross appearance: brown goo replaces fat.
Histology
General
It's the at the pathologists discretion. In decomp cases it is reasonable to submit nothing.
Forensic context
A standard (minimum) for adult homicides is:
Hospital autopsies
Non-neuropathology
A standard based on a Toronto teaching hospital:
- Thyroid gland (1).
- Lung - each lobe (5).
- Heart - posterior papillary muscle & LV, anterior papillary muscle & LV (2).
- More extensive histologic sectioning is discussed in the heart article.
- Liver - left lobe, right lobe (2).
- Spleen - including hilum & capsule (1).
- Adrenal gland (1).
- Gastrointestinal tract:
- The quality is often very poor (even in "fresh" bodies). These are often omitted.
- Pancreas - head & tail (1).
- Stomach (1).
- Esophagus (1).
- Small bowel (1).
- Large bowel (1).
- The quality is often very poor (even in "fresh" bodies). These are often omitted.
- Genitourinary tract:
- Kidney - each side (2).
- Gender specific:
- Male:
- Prostate gland (1).
- Testis (1).
- Female:
- Male:
- Bone marrow (1).
Neuro
- Pituitary gland (1).
- Cortex usu. frontal/parietal (1).
- Hippocampus (1).
- Cerebellum (1).
- Brain stem (1).
- Basal ganglia (1).
Stock
- Thyroid gland.
- Heart:
- Complete (axial) slice (including RV and LV).
- Tissue with SA node.
- Tissue with AV node.
- Lung - all five lobes.
- Spleen.
- Urinary:
- Kidney.
- Urinary bladder.
- Gastrointestinal tract:
- Reproductive:
- Male:
- Female:
- Neurologic:
- Hippocampus + basal ganglia.
- Cortex.
- Brainstem.
- Cerebellum.
- Skin.
- Nerve.
- Muscle.
- Lymph nodes.
Autopsy report
Normal size parameters
Normal organ masses (adult)
Caucasoid population of 684 adults:[36]
| Men | Women | |
| Heart | 365 +/- 71 g | 312 +/- 78 g |
| Right lung | 663 +/- 239 g | 546 +/- 207 g |
| Left lung | 583 +/- 216 g | 467 +/- 174 g |
| Liver | 1677 +/- 396 g | 1475 +/- 362 g |
| Spleen | 156 +/- 87 g | 140 +/- 78 g |
| Right kidney | 162 +/- 39 g | 135 +/- 39 g |
| Left kidney | 160 +/- 41 g | 136 +/- 37 g |
Pediatrics
Negative autopsy
Definition:
- A negative autopsy is a post-mortem exam that has no anatomical or toxicological cause of death.
- This does not preclude the presence of pathology (that is not sufficient to cause death).
Cause of death (in a negative autopsy):
- Unascertained.
Considerations
- Channelopathy - may be elucidated by molecular testing.
- Electrocution (unrecognized).
- Decomposition.
- Sudden Unexpected Death in Epilepsy (SUDEP)[37] - missing history.
- Sudden infant death syndrome.
Histology checklist
| Section/organ | Expected finding(s)/common finding(s) | Findings to consider |
|---|---|---|
| Bone marrow |
|
|
| Coronary arteries |
|
|
| Heart muscle |
|
|
| Adrenal gland |
|
|
| Kidney |
|
|
| Liver |
|
|
| Spleen |
|
|
| Gastrointestinal tract |
|
|
| Thyroid gland |
|
|
| Lung |
|
|
List form
Bone marrow
- Trilineage hematopoiesis present.
- Negative for infection and negative for tumour.
Cardiovascular system
- Atherosclerosis in the:
- Left main coronary artery.
- Left anterior descending coronary artery.
- Left circumflex coronary artery.
- Right coronary artery.
- No identified atherosclerotic plaque rupture.
- No thrombosis.
- No vasculitis.
Heart muscle:
- Fibrosis - posterior left ventricle.
- Nuclear enlargement, arteriolosclerosis and periarteriolar fibrosis.
- No hemorrhage.
- No wavy fibres.
- No necrosis.
- No inflammatory infiltrate.
- No hyaline material.
Endocrine organs
- No pathology apparent.
- No tumour.
- No hemorrhage.
- No fatty replacement.
Thyroid gland:
- Normal thyroid gland.
- No tumour.
- No inflammation.
Genitourinary system
- Atherosclerosis, mild.
- Arteriolar hyalinization.
- No tumour.
- Normal glomeruli (no enlargement, no crescents, no mesangial expansion, no inflammation).
- No thrombi.
- No interstitial fibrosis, no inflammation, and no edema.
- No tubular inflammation, no whorls, and no fragmentation.
- No apparently pathologic renal casts.
Gastrointestinal system
- Steatosis - mild, centrilobular, macrovesicular.
- No fibrosis.
- No inflammation.
- No tumour.
- Normal bile ducts.
- No ballooning degeneration and no feathery degeneration.
- No necrosis.
Luminal GI tract:
- Autolytic changes.
- No tumour
- No vasculitis.
- No siginificant atherosclerosis.
- No inflammation.
- No fibrosis.
Spleen
- Normal white pulp/red pulp.
- No tumour.
- No surface abnormalities.
Lung
- Pulmonary edema.
- Infectious pneumonia, mild.
- Emphysema, mild.
- No pulmonary hypertension.
- No interstitial fibrosis.
- No tumour,
- No granulomas,
- No significant hemorrhage.
- No hyaline membranes.
Sign out
Sample clinical history
A 63 year old male with a history of alcohol abuse was admitted on December 13, 2022 for recurrent alcohol related pancreatitis. On December 21, he was found unresponsive at 0:15. Approximately fifteen minutes earlier, he was on oxygen and in no apparent distress. A code blue was called; however, the attempted resuscitation was unsuccessful. Death was declared at 1:00 on December 21, 2022.
See also
References
- ↑ Roulson, J.; Benbow, EW.; Hasleton, PS. (Dec 2005). "Discrepancies between clinical and autopsy diagnosis and the value of post mortem histology; a meta-analysis and review.". Histopathology 47 (6): 551-9. doi:10.1111/j.1365-2559.2005.02243.x. PMID 16324191.
- ↑ Brian Gallagher, Burton EC, McDonald KM, Goldman L (2003). "Changes in rates of autopsy-detected diagnostic errors over time: a systematic review". JAMA 289 (21): 2849–56. doi:10.1001/jama.289.21.2849. PMID 12783916.
- ↑ 3.0 3.1 URL: http://www.docstoc.com/docs/51609856/CONSENT-FOR-AUTOPSY. Accessed on: 27 September 2010.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 43. ISBN 978-0340965146.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 47. ISBN 978-0340965146.
- ↑ Siebert, JR. (Dec 2009). "Increasing the efficiency of autopsy reporting.". Arch Pathol Lab Med 133 (12): 1932-7. doi:10.1043/1543-2165-133.12.1932. PMID 19961247.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 101. ISBN 978-0340965146.
- ↑ TR. 28 September 2010.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 120-1. ISBN 978-0340965146.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 118. ISBN 978-0340965146.
- ↑ Fokin AA (May 2000). "Cleft sternum and sternal foramen". Chest Surg. Clin. N. Am. 10 (2): 261–76. PMID 10803333.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 156. ISBN 978-0340965146.
- ↑ URL: http://www.meddean.luc.edu/lumen/meded/mech/cases/case1/list.htm. Accessed on 8 October 2010.
- ↑ URL: http://www.elsevier.es/cardio_eng/ctl_servlet?_f=40&ident=13142654. Accessed on: 8 October 2010.
- ↑ Püschel, K.; Schulz, F.; Darrmann, I.; Tsokos, M. (1999). "Macromorphology and histology of intramuscular hemorrhages in cases of drowning.". Int J Legal Med 112 (2): 101-6. PMID 10048667.
- ↑ Di Nunno N, Lombardo S, Costantinides F, Di Nunno C (March 2004). "Anomalies and alterations of the hyoid-larynx complex in forensic radiographic studies". Am J Forensic Med Pathol 25 (1): 14–9. PMID 15075682.
- ↑ URL: http://faculty.ksu.edu.sa/Prof.Hamam/curses/Jurnals%20Club/225-Triticeous%20cartilage.pdf. Accessed on: 10 September 2010.
- ↑ URL: http://medical-dictionary.thefreedictionary.com/triticeous. Accessed on: 15 September 2010.
- ↑ Evgenij Gazov. LMU Rechtsmedizin. 8 July 2011. Possibly described more here: http://www.reference-global.com/doi/abs/10.1515/9783899496079.1027
- ↑ Ali-Ridha, HN. 8 October 2010.
- ↑ 21.0 21.1 Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 156. ISBN 978-0340965146.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 90. ISBN 978-0521868792.
- ↑ Barzon L, Sonino N, Fallo F, Palu G, Boscaro M (October 2003). "Prevalence and natural history of adrenal incidentalomas". Eur. J. Endocrinol. 149 (4): 273–85. PMID 14514341.
- ↑ Yamagawa, H.; Onishi, T. (Sep 1989). "[A clinicopathological study of early gastric cancers with a diameter larger than five centimeters].". Gan No Rinsho 35 (10): 1114-8. PMID 2550682.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 140. ISBN 978-0340965146.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 138. ISBN 978-0340965146.
- ↑ Glodny, B.; Unterholzner, V.; Taferner, B.; Hofmann, KJ.; Rehder, P.; Strasak, A.; Petersen, J. (2009). "Normal kidney size and its influencing factors - a 64-slice MDCT study of 1.040 asymptomatic patients.". BMC Urol 9: 19. doi:10.1186/1471-2490-9-19. PMID 20030823.
- ↑ Ono, H.; Ono, Y. (Nov 1997). "Nephrosclerosis and hypertension.". Med Clin North Am 81 (6): 1273-88. PMID 9356598.
- ↑ Kocovski, L.; Duflou, J. (Mar 2009). "Can renal acute tubular necrosis be differentiated from autolysis at autopsy?". J Forensic Sci 54 (2): 439-42. doi:10.1111/j.1556-4029.2008.00956.x. PMID 19207286.
- ↑ Burton, Julian L.; Rutty, Guy N. (2010). The Hospital Autopsy A Manual of Fundamental Autopsy Practice (3rd ed.). Oxford University Press. pp. 130. ISBN 978-0340965146.
- ↑ Ramos GA, Ylagan MV, Romine LE, D'Agostini DA, Pretorius DH (December 2008). "Diagnostic evaluation of the fetal face using 3-dimensional ultrasound". Ultrasound Q 24 (4): 215–23. doi:10.1097/RUQ.0b013e31819073c2. PMID 19060688.
- ↑ Heemskerk, S.; van Haren, FM.; Foudraine, NA.; Peters, WH.; van der Hoeven, JG.; Russel, FG.; Masereeuw, R.; Pickkers, P. (Feb 2008). "Short-term beneficial effects of methylene blue on kidney damage in septic shock patients.". Intensive Care Med 34 (2): 350-4. doi:10.1007/s00134-007-0867-9. PMID 17926021.
- ↑ Tan, CD.; Rodriguez, ER.. "Blue dye, green heart.". Cardiovasc Pathol 19 (2): 125-6. doi:10.1016/j.carpath.2008.06.012. PMID 18703358.
- ↑ http://cat.inist.fr/?aModele=afficheN&cpsidt=18942659
- ↑ KC. 14 September 2010.
- ↑ de la Grandmaison GL, Clairand I, Durigon M (June 2001). "Organ weight in 684 adult autopsies: new tables for a Caucasoid population". Forensic Sci. Int. 119 (2): 149–54. PMID 11376980.
- ↑ URL: http://emedicine.medscape.com/article/1187111-overview. Accessed on: 11 October 2010.