Difference between revisions of "Parathyroid adenoma"
(→Weight) |
|||
| (19 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Parathyroid adenoma intermed mag.jpg | |||
| Width = | |||
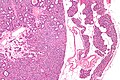
| Caption = Chief cell parathyroid adenoma (left of image) and unremarkable parathyroid gland (right of image). [[H&E stain]]. (WC) | |||
| Synonyms = | |||
| Micro = proliferation of parathyroid cells (chief cells, oxyphils or both) usually lacking adipose tissue, +/-rimmed by normal parathyroid gland, lack of destructive invasion of surround structures, lack of metastatic disease | |||
| Subtypes = chief cell, oxyphil, mixed | |||
| LMDDx = [[parathyroid hyperplasia]], [[parathyroid carcinoma]], [[lymph node]], [[thyroid gland]], [[Hürthle cell adenoma]] of thyroid (for ''oxyphil'' subtype) | |||
| Stains = | |||
| IHC = Ki-67 low | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = [[parathyroid gland]] ([[head and neck pathology|neck]]/[[mediastinum]]) | |||
| Assdx = [[nephrolithiasis|renal stones]], osteitis fibrosa cystica | |||
| Syndromes = [[MEN 1|multiple endocrine neoplasia 1]], [[MEN 2A|multiple endocrine neoplasia 2A]] | |||
| Clinicalhx = | |||
| Signs = constipation | |||
| Symptoms = bone pain, abdominal pain, lethargy, fatigue, memory loss | |||
| Prevalence = | |||
| Bloodwork = increased parathyroid hormone, serum calcium increased | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = benign | |||
| Other = depression, psychosis, delirium, coma, ataxia | |||
| ClinDDx = nodule (lymph node, other tumours), hyperparathyroidism ([[parathyroid hyperplasia]], [[parathyroid carcinoma]]), DDx of [[hypercalcemia]] | |||
| Tx = surgical excision | |||
}} | |||
'''Parathyroid adenoma''' is a common benign pathology of the [[parathyroid gland]]. | '''Parathyroid adenoma''' is a common benign pathology of the [[parathyroid gland]]. | ||
==General== | ==General== | ||
*[[Clinical diagnosis]]. | *[[Clinical diagnosis]] - significant intraoperative drop of PTH after removal of suspected adenoma.<ref name=pmid26211860>{{Cite journal | last1 = Özkul | first1 = MH. | last2 = Uyar | first2 = M. | last3 = Bayram | first3 = Ö. | last4 = Dikmen | first4 = B. | title = Parathyroid scintigraphy and minimal invasive surgery in parathyroid adenomas. | journal = Kulak Burun Bogaz Ihtis Derg | volume = 25 | issue = 4 | pages = 205-13 | month = | year = | doi = | PMID = 26211860 }}</ref> | ||
*Most common cause of [[primary hyperparathyroidism]].<ref name=Ref_PBoD8_1127>{{Ref PBoD8|1127}}</ref> | |||
*May be associated with [[MEN 1]] | *May be associated with [[MEN 1]] or [[MEN 2A]]. | ||
MEN 1: | MEN 1: | ||
| Line 23: | Line 54: | ||
#*Uncommon.<ref name=pmid15579742>{{Cite journal | last1 = Fleischer | first1 = J. | last2 = Becker | first2 = C. | last3 = Hamele-Bena | first3 = D. | last4 = Breen | first4 = TL. | last5 = Silverberg | first5 = SJ. | title = Oxyphil parathyroid adenoma: a malignant presentation of a benign disease. | journal = J Clin Endocrinol Metab | volume = 89 | issue = 12 | pages = 5948-51 | month = Dec | year = 2004 | doi = 10.1210/jc.2004-1597 | PMID = 15579742 }}</ref> | #*Uncommon.<ref name=pmid15579742>{{Cite journal | last1 = Fleischer | first1 = J. | last2 = Becker | first2 = C. | last3 = Hamele-Bena | first3 = D. | last4 = Breen | first4 = TL. | last5 = Silverberg | first5 = SJ. | title = Oxyphil parathyroid adenoma: a malignant presentation of a benign disease. | journal = J Clin Endocrinol Metab | volume = 89 | issue = 12 | pages = 5948-51 | month = Dec | year = 2004 | doi = 10.1210/jc.2004-1597 | PMID = 15579742 }}</ref> | ||
#Mixed. | #Mixed. | ||
==Gross== | |||
*One parathyroid gland is big... the others are small. | |||
Note: | |||
*There is a classification system by Perrier ''et al.'' that may be seen in radiology reports to describe the position of an adenoma.<ref name=pmid19148701>{{Cite journal | last1 = Perrier | first1 = ND. | last2 = Edeiken | first2 = B. | last3 = Nunez | first3 = R. | last4 = Gayed | first4 = I. | last5 = Jimenez | first5 = C. | last6 = Busaidy | first6 = N. | last7 = Potylchansky | first7 = E. | last8 = Kee | first8 = S. | last9 = Vu | first9 = T. | title = A novel nomenclature to classify parathyroid adenomas. | journal = World J Surg | volume = 33 | issue = 3 | pages = 412-6 | month = Mar | year = 2009 | doi = 10.1007/s00268-008-9894-0 | PMID = 19148701 }}</ref> | |||
===Weight=== | |||
It is common practice to weight parathyroid tissue: | |||
*Parathyroid adenoma are: 0.55 +/- 0.52 grams.<ref name=pmid15240594>{{Cite journal | last1 = Yao | first1 = K. | last2 = Singer | first2 = FR. | last3 = Roth | first3 = SI. | last4 = Sassoon | first4 = A. | last5 = Ye | first5 = C. | last6 = Giuliano | first6 = AE. | title = Weight of normal parathyroid glands in patients with parathyroid adenomas. | journal = J Clin Endocrinol Metab | volume = 89 | issue = 7 | pages = 3208-13 | month = Jul | year = 2004 | doi = 10.1210/jc.2003-031184 | PMID = 15240594 }}</ref> | |||
*Normal parathyroids taken out with parathyroid adenomas are: 0.06 +/-0.03 grams.<ref name=pmid15240594/> | |||
==Microscopic== | ==Microscopic== | ||
Features | Features: | ||
*Proliferation of parathyroid cells (chief cells, oxyphils or both) lacking adipose tissue. | *Proliferation of parathyroid cells (chief cells, oxyphils or both) usually intermixed lacking adipose tissue. | ||
* | *+/-Rim of normal parathyroid gland around the lesion<ref name=Ref_BITFS191>{{Ref BITFS|191}}</ref> with adipose tissue. | ||
Note: | Note: | ||
*Generally, it is impossible to discern between [[parathyroid adenoma]]s and [[parathyroid hyperplasia]]s by histology alone.<ref name=Ref_BITFS191>{{Ref BITFS|191}}</ref> | *Generally, it is impossible to discern between [[parathyroid adenoma]]s and [[parathyroid hyperplasia]]s by histology alone.<ref name=Ref_BITFS191>{{Ref BITFS|191}}</ref> | ||
**One requires information | **One requires information on the size of the other glands to make the [[diagnosis]]. | ||
**Ideally, histologic findings should be correlated with the PTH serology. | |||
DDx: | DDx: | ||
*[[Parathyroid hyperplasia]] - differentiated by clinical history. | *[[Parathyroid hyperplasia]] - differentiated by clinical history. | ||
*[[Parathyroid carcinoma]] - destructive invasion of surrounding tissue or far away mets, increased proliferative activity. | *[[Parathyroid carcinoma]] - destructive invasion of surrounding tissue or far away mets, increased proliferative activity. | ||
*[[Lymph node]]. | |||
*[[Hürthle cell adenoma]] - for oxyphil type (see below). | |||
*[[Thyroid gland]]. | |||
===Chief cell parathyroid adenoma=== | ===Chief cell parathyroid adenoma=== | ||
| Line 65: | Line 111: | ||
*[[Hürthle cell adenoma]] of the [[thyroid gland]]. | *[[Hürthle cell adenoma]] of the [[thyroid gland]]. | ||
Image: | ====Image==== | ||
<gallery> | |||
Image: Oxyphil parathyroid adenoma -- low mag.jpg | Oxyphil PA - low mag. (WC) | |||
Image: Oxyphil parathyroid adenoma -- intermed mag.jpg | Oxyphil PA - intermed. mag. (WC) | |||
Image: Oxyphil parathyroid adenoma - alt -- intermed mag.jpg | Oxyphil PA - intermed. mag. (WC) | |||
Image: Oxyphil parathyroid adenoma - high mag.jpg | Oxyphil PA - high mag. (WC) | |||
Image: Oxyphil parathyroid adenoma - very high mag.jpg | Oxyphil PA - very high mag. (WC) | |||
</gallery> | |||
<gallery> | |||
Image: Parathyroid adenoma, mixed type -- high mag.jpg | PA, mixed type - high mag. (WC) | |||
Image: Parathyroid adenoma, mixed type -- very high mag.jpg | PA, mixed type - very high mag. (WC) | |||
Image: Parathyroid adenoma - oxyphil cells -- high mag.jpg | Oxyphil cells - high mag. (WC) | |||
</gallery> | |||
=====www===== | |||
*[http://library.med.utah.edu/WebPath/jpeg4/ENDO091.jpg Parathyroid adenoma (med.utah.edu)].<ref>URL: [http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html]. Accessed on: 6 December 2010.</ref> | *[http://library.med.utah.edu/WebPath/jpeg4/ENDO091.jpg Parathyroid adenoma (med.utah.edu)].<ref>URL: [http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html]. Accessed on: 6 December 2010.</ref> | ||
| Line 72: | Line 131: | ||
*One should not say "negative for malignancy". | *One should not say "negative for malignancy". | ||
<pre> | |||
Parathyroid Gland (Submitted as "Right Superior Parathyroid Adenoma"), Excision: | |||
- Parathyroid adenoma with adjacent normal parathyroid tissue. | |||
</pre> | |||
===Chief cell type=== | |||
<pre> | <pre> | ||
Parathyroid Gland, Excision: | Parathyroid Gland, Excision: | ||
| Line 82: | Line 147: | ||
</pre> | </pre> | ||
===Oxyphil type=== | |||
<pre> | |||
Right Superior Parathyroid, Excision: | |||
- Consistent with parathyroid adenoma (oxyphil type) with rim of | |||
normal appearing parathyroid tissue. | |||
</pre> | |||
====Tertiary hyperparathyroidism==== | |||
<pre> | |||
A. Right Inferior Parathyroid, Excision: | |||
- Cellular parathyroid tissue with a rim of normal-appearing | |||
parathyroid tissue, compatible with parathyroid adenoma. | |||
B. Portion of Right Superior Parathyroid, Excision: | |||
- Cellular parathyroid compatible with adenoma or hyperplasia. | |||
</pre> | |||
====Unclear history==== | |||
<pre> | <pre> | ||
Submitted as "Right Inferior Parathyroid", Excision: | |||
- | - Hyperplastic appearing parathyroid tissue devoid of fat consisting of a | ||
mixture of chief cells and oncocytic cells, compatible with parathyroid | |||
adenoma in proper clinical context. | |||
- Unremarkable parathyroid tissue. | |||
</pre> | </pre> | ||
====Block letters==== | ====Block letters==== | ||
<pre> | <pre> | ||
PARATHYROID GLAND, EXCISION: | |||
- CHIEF CELL PARATHYROID ADENOMA. | - CHIEF CELL PARATHYROID ADENOMA. | ||
</pre> | </pre> | ||
Latest revision as of 16:44, 17 October 2019
| Parathyroid adenoma | |
|---|---|
| Diagnosis in short | |
 Chief cell parathyroid adenoma (left of image) and unremarkable parathyroid gland (right of image). H&E stain. (WC) | |
|
| |
| LM | proliferation of parathyroid cells (chief cells, oxyphils or both) usually lacking adipose tissue, +/-rimmed by normal parathyroid gland, lack of destructive invasion of surround structures, lack of metastatic disease |
| Subtypes | chief cell, oxyphil, mixed |
| LM DDx | parathyroid hyperplasia, parathyroid carcinoma, lymph node, thyroid gland, Hürthle cell adenoma of thyroid (for oxyphil subtype) |
| IHC | Ki-67 low |
| Site | parathyroid gland (neck/mediastinum) |
|
| |
| Associated Dx | renal stones, osteitis fibrosa cystica |
| Syndromes | multiple endocrine neoplasia 1, multiple endocrine neoplasia 2A |
|
| |
| Signs | constipation |
| Symptoms | bone pain, abdominal pain, lethargy, fatigue, memory loss |
| Blood work | increased parathyroid hormone, serum calcium increased |
| Prognosis | benign |
| Other | depression, psychosis, delirium, coma, ataxia |
| Clin. DDx | nodule (lymph node, other tumours), hyperparathyroidism (parathyroid hyperplasia, parathyroid carcinoma), DDx of hypercalcemia |
| Treatment | surgical excision |
Parathyroid adenoma is a common benign pathology of the parathyroid gland.
General
- Clinical diagnosis - significant intraoperative drop of PTH after removal of suspected adenoma.[1]
- Most common cause of primary hyperparathyroidism.[2]
- May be associated with MEN 1 or MEN 2A.
MEN 1:
- Parathyroid adenoma.
- Pancreatic neuroendocrine tumour.
- Pituitary adenoma.
MEN 2A:
- Parathyroid adenoma.
- Medullary thyroid carcinoma.
- Pheochromocytoma.
Subtypes
Histologic subtyping:[3]
- Chief cell parathyroid adenoma.
- Common.
- Oxyphil parathyroid adenoma.
- Uncommon.[4]
- Mixed.
Gross
- One parathyroid gland is big... the others are small.
Note:
- There is a classification system by Perrier et al. that may be seen in radiology reports to describe the position of an adenoma.[5]
Weight
It is common practice to weight parathyroid tissue:
- Parathyroid adenoma are: 0.55 +/- 0.52 grams.[6]
- Normal parathyroids taken out with parathyroid adenomas are: 0.06 +/-0.03 grams.[6]
Microscopic
Features:
- Proliferation of parathyroid cells (chief cells, oxyphils or both) usually intermixed lacking adipose tissue.
- +/-Rim of normal parathyroid gland around the lesion[7] with adipose tissue.
Note:
- Generally, it is impossible to discern between parathyroid adenomas and parathyroid hyperplasias by histology alone.[7]
- One requires information on the size of the other glands to make the diagnosis.
- Ideally, histologic findings should be correlated with the PTH serology.
DDx:
- Parathyroid hyperplasia - differentiated by clinical history.
- Parathyroid carcinoma - destructive invasion of surrounding tissue or far away mets, increased proliferative activity.
- Lymph node.
- Hürthle cell adenoma - for oxyphil type (see below).
- Thyroid gland.
Chief cell parathyroid adenoma
Features:[2]
- Chief cells - key feature:
- Small central nucleus.
- Round with stippled chromatin - important.
- Moderate cytoplasm.
- Small central nucleus.
- +/-Scattered oxyphil cells:
- Large cells.
- Abundant cytoplasm.
- Architecture:
- Nests.
- Circular formations - often around capillaries (perivascular pseudorosettes).
Images
Parathyroid adenoma - low mag. (WC/Nephron)

Parathyroid adenoma - high mag. (WC/Nephron)


Oxyphil parathyroid adenoma
Features:[2]
- Oxyphil cells:
- Large cells.
- Abundant cytoplasm.
DDx:
- Hürthle cell adenoma of the thyroid gland.
Image

Oxyphil PA - low mag. (WC)

Oxyphil PA - intermed. mag. (WC)

Oxyphil PA - intermed. mag. (WC)

Oxyphil PA - high mag. (WC)

Oxyphil PA - very high mag. (WC)






PA, mixed type - high mag. (WC)

PA, mixed type - very high mag. (WC)

Oxyphil cells - high mag. (WC)



www
{kind=link}
Sign out
Note:
- One should not say "negative for malignancy".
Parathyroid Gland (Submitted as "Right Superior Parathyroid Adenoma"), Excision: - Parathyroid adenoma with adjacent normal parathyroid tissue.
Chief cell type
Parathyroid Gland, Excision: - Chief cell parathyroid adenoma.
Parathyroid Gland, Excision: - Chief cell parathyroid adenoma with adjacent normal parathyroid tissue.
Oxyphil type
Right Superior Parathyroid, Excision: - Consistent with parathyroid adenoma (oxyphil type) with rim of normal appearing parathyroid tissue.
Tertiary hyperparathyroidism
A. Right Inferior Parathyroid, Excision: - Cellular parathyroid tissue with a rim of normal-appearing parathyroid tissue, compatible with parathyroid adenoma. B. Portion of Right Superior Parathyroid, Excision: - Cellular parathyroid compatible with adenoma or hyperplasia.
Unclear history
Submitted as "Right Inferior Parathyroid", Excision: - Hyperplastic appearing parathyroid tissue devoid of fat consisting of a mixture of chief cells and oncocytic cells, compatible with parathyroid adenoma in proper clinical context. - Unremarkable parathyroid tissue.
Block letters
PARATHYROID GLAND, EXCISION: - CHIEF CELL PARATHYROID ADENOMA.
Micro
The section shows an adenoma consisting predominantly of chief cells. A rim of normal parathyroid is seen adjacent to the adenoma. A small amount of unremarkable adipose tissue is present.
See also
References
- ↑ Özkul, MH.; Uyar, M.; Bayram, Ö.; Dikmen, B.. "Parathyroid scintigraphy and minimal invasive surgery in parathyroid adenomas.". Kulak Burun Bogaz Ihtis Derg 25 (4): 205-13. PMID 26211860.
- ↑ 2.0 2.1 2.2 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1127. ISBN 978-1416031215.
- ↑ Moran, CA.; Suster, S. (Nov 2005). "Primary parathyroid tumors of the mediastinum: a clinicopathologic and immunohistochemical study of 17 cases.". Am J Clin Pathol 124 (5): 749-54. doi:10.1309/WJEL-N05L-9A06-9DU0. PMID 16203274.
- ↑ Fleischer, J.; Becker, C.; Hamele-Bena, D.; Breen, TL.; Silverberg, SJ. (Dec 2004). "Oxyphil parathyroid adenoma: a malignant presentation of a benign disease.". J Clin Endocrinol Metab 89 (12): 5948-51. doi:10.1210/jc.2004-1597. PMID 15579742.
- ↑ Perrier, ND.; Edeiken, B.; Nunez, R.; Gayed, I.; Jimenez, C.; Busaidy, N.; Potylchansky, E.; Kee, S. et al. (Mar 2009). "A novel nomenclature to classify parathyroid adenomas.". World J Surg 33 (3): 412-6. doi:10.1007/s00268-008-9894-0. PMID 19148701.
- ↑ 6.0 6.1 Yao, K.; Singer, FR.; Roth, SI.; Sassoon, A.; Ye, C.; Giuliano, AE. (Jul 2004). "Weight of normal parathyroid glands in patients with parathyroid adenomas.". J Clin Endocrinol Metab 89 (7): 3208-13. doi:10.1210/jc.2003-031184. PMID 15240594.
- ↑ 7.0 7.1 Taxy, J.; Husain, A; Montag, A. (2009). Biopsy Interpretation: The Frozen Section (1st ed.). Lippincott Williams & Wilkins. pp. 191. ISBN 978-0781767798.
- ↑ URL: http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/enfrm.html. Accessed on: 6 December 2010.