Difference between revisions of "Adenocarcinoma of the uterine cervix"
Jump to navigation
Jump to search
(→IHC) |
|||
| (6 intermediate revisions by the same user not shown) | |||
| Line 33: | Line 33: | ||
It is also known as '''endocervical adenocarcinoma''' and '''cervical adenocarcinoma'''. | It is also known as '''endocervical adenocarcinoma''' and '''cervical adenocarcinoma'''. | ||
Very well-differentiated adenocarcinoma of the cervix is covered in ''[[minimal deviation adenocarcinoma of the uterine cervix]]''. | |||
==General== | ==General== | ||
*Adenocarcinoma of the cervix is much less common than squamous dysplasia of the cervix/SCC of the cervix. | *Adenocarcinoma of the cervix is much less common than squamous dysplasia of the cervix/SCC of the cervix. | ||
*Arises from the endocervical glands. | *Arises from the endocervical glands. | ||
*Usually [[HPV]] related. | |||
*Non-HPV related adenocarcinoma may be syndromic - [[Peutz-Jeghers syndrome]], [[Li-Fraumeni syndrome]].<ref name=pmid26457350>{{Cite journal | last1 = Karamurzin | first1 = YS. | last2 = Kiyokawa | first2 = T. | last3 = Parkash | first3 = V. | last4 = Jotwani | first4 = AR. | last5 = Patel | first5 = P. | last6 = Pike | first6 = MC. | last7 = Soslow | first7 = RA. | last8 = Park | first8 = KJ. | title = Gastric-type Endocervical Adenocarcinoma: An Aggressive Tumor With Unusual Metastatic Patterns and Poor Prognosis. | journal = Am J Surg Pathol | volume = 39 | issue = 11 | pages = 1449-57 | month = Nov | year = 2015 | doi = 10.1097/PAS.0000000000000532 | PMID = 26457350 }}</ref> | |||
==Microscopic== | ==Microscopic== | ||
| Line 71: | Line 75: | ||
Image:Cervical_adenocarcinoma_-_intermed_mag.jpg | Cervical adenocarcinoma - intermed. mag. (WC) | Image:Cervical_adenocarcinoma_-_intermed_mag.jpg | Cervical adenocarcinoma - intermed. mag. (WC) | ||
Image:Cervical_adenocarcinoma_-_high_mag.jpg | Cervical adenocarcinoma - high mag. (WC) | Image:Cervical_adenocarcinoma_-_high_mag.jpg | Cervical adenocarcinoma - high mag. (WC) | ||
</gallery> | |||
<gallery> | |||
Image: Endocervical_adenocarcinoma_(1).jpg | Endocervical adenocarcinoma. (WC/KGH) | |||
Image: Endocervical_adenocarcinoma_(2).jpg | Endocervical adenocarcinoma. (WC/KGH) | |||
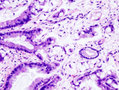
Image: Endocervical_adenocarcinoma_(3).jpg | Endocervical adenocarcinoma. (WC/KGH) | |||
Image: Endocervical_adenocarcinoma_(4).jpg | Endocervical adenocarcinoma. (WC/KGH) | |||
</gallery> | </gallery> | ||
| Line 76: | Line 86: | ||
Features for diagnosis: | Features for diagnosis: | ||
*p16 +ve. | *p16 +ve. | ||
**May be negative ~25% of cases in one series.<ref name=pmid23626605>{{Cite journal | last1 = Izadi-Mood | first1 = N. | last2 = Asadi | first2 = K. | last3 = Shojaei | first3 = H. | last4 = Sarmadi | first4 = S. | last5 = Ahmadi | first5 = SA. | last6 = Sani | first6 = S. | last7 = Chelavi | first7 = LH. | title = Potential diagnostic value of P16 expression in premalignant and malignant cervical lesions. | journal = J Res Med Sci | volume = 17 | issue = 5 | pages = 428-33 | month = May | year = 2012 | doi = | PMID = 23626605 }}</ref> | |||
*Ki-67 -- high. | *Ki-67 -- high. | ||
Uterus vs. cervix:<ref> | Uterus vs. cervix:<ref name=pmid20335127>{{Cite journal | last1 = Hu | first1 = WW. | last2 = Tao | first2 = JH. | last3 = Li | first3 = GM. | last4 = Xu | first4 = X. | last5 = Yang | first5 = XM. | title = [Value of ER, VIM, CEA and p16 detection in the diagnosis and differential diagnosis of primary endocervical and endometrial adenocarcinomas]. | journal = Nan Fang Yi Ke Da Xue Xue Bao | volume = 30 | issue = 3 | pages = 526-8, 531 | month = Mar | year = 2010 | doi = | PMID = 20335127 }}</ref> | ||
*Cervix (typically): CEA +ve, p16 +ve. | *Cervix (typically): CEA +ve, p16 +ve. | ||
**ER -ve, PR -ve, vimentin -ve. | **[[ER]] -ve, PR -ve, vimentin -ve. | ||
*Uterus (typically): vimentin +ve, ER +ve, PR +ve. | *Uterus (typically): vimentin +ve, ER +ve, PR +ve. | ||
**CEA -ve, p16 -ve. | **CEA -ve, p16 -ve. | ||
Latest revision as of 20:34, 23 June 2016
| Adenocarcinoma of the uterine cervix | |
|---|---|
| Diagnosis in short | |
 Cervical adenocarcinoma. H&E stain. | |
| LM DDx | microglandular hyperplasia, endocervical adenocarcinoma in situ, metastatic adenocarcinoma (e.g. endometrioid endometrial carcinoma, serous endometrial carcinoma, colorectal adenocarcinoma), villoglandular adenocarcinoma, glassy cell carcinoma, clear cell carcinoma of the cervix |
| IHC | p16 +ve, CEA +ve, vimentin -ve, ER -ve, PR -ve |
| Site | uterine cervix - endocervical canal |
|
| |
| Prevalence | uncommon |
| Prognosis | fairly good |
| Clin. DDx | other cervical tumours |
| Treatment | radical trachelectomy or radical hysterectomy |
Adenocarcinoma of the uterine cervix is a relative uncommon form of cervical cancer. Like the more common squamous cell carcinoma, it is associated strongly with the human papilloma virus.
It is also known as endocervical adenocarcinoma and cervical adenocarcinoma.
Very well-differentiated adenocarcinoma of the cervix is covered in minimal deviation adenocarcinoma of the uterine cervix.
General
- Adenocarcinoma of the cervix is much less common than squamous dysplasia of the cervix/SCC of the cervix.
- Arises from the endocervical glands.
- Usually HPV related.
- Non-HPV related adenocarcinoma may be syndromic - Peutz-Jeghers syndrome, Li-Fraumeni syndrome.[1]
Microscopic
Features:
- Cells with moderate cytoplasm, typically with basally stratfied nuclei.
- Cytologic changes:
- Nuclear hyperchromasia.
- Nuclear pseudostratification.
- Nuclear enlargement.
- Stromal changes - "desmoplastic stroma/desmoplastic reaction".
- Fibrosis/streaming cells.
- Abnormal architecture:
- Gland fusion.
- Glands too deep -- very fuzzy criterion.
Notes:
- AIS changes - similar to colonic dysplasia.
- AIS may occur together with CIN.
- Not infrequently they (AIS, CIN) occur together - both are due, indirectly, to HPV infection.
- May be difficult to be certain of invasion.
- A feature suggestive of invasion is cytoplasmic eosinophilia.
DDx:
- Microglandular hyperplasia - NC ratio normal, no nuclear atypia.
- Endocervical adenocarcinoma in situ.
- Villoglandular adenocarcinoma.
- Glassy cell carcinoma.
- Metastatic adenocarcinoma.
Images

Cervical adenocarcinoma - low mag. (WC)

Cervical adenocarcinoma - intermed. mag. (WC)

Cervical adenocarcinoma - high mag. (WC)


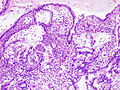
Endocervical adenocarcinoma. (WC/KGH)
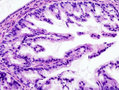
Endocervical adenocarcinoma. (WC/KGH)

Endocervical adenocarcinoma. (WC/KGH)
Endocervical adenocarcinoma. (WC/KGH)
.jpg)
.jpg)
.jpg)
.jpg)
IHC
Features for diagnosis:
- p16 +ve.
- May be negative ~25% of cases in one series.[2]
- Ki-67 -- high.
Uterus vs. cervix:[3]
- Cervix (typically): CEA +ve, p16 +ve.
- ER -ve, PR -ve, vimentin -ve.
- Uterus (typically): vimentin +ve, ER +ve, PR +ve.
- CEA -ve, p16 -ve.
See also
References
- ↑ Karamurzin, YS.; Kiyokawa, T.; Parkash, V.; Jotwani, AR.; Patel, P.; Pike, MC.; Soslow, RA.; Park, KJ. (Nov 2015). "Gastric-type Endocervical Adenocarcinoma: An Aggressive Tumor With Unusual Metastatic Patterns and Poor Prognosis.". Am J Surg Pathol 39 (11): 1449-57. doi:10.1097/PAS.0000000000000532. PMID 26457350.
- ↑ Izadi-Mood, N.; Asadi, K.; Shojaei, H.; Sarmadi, S.; Ahmadi, SA.; Sani, S.; Chelavi, LH. (May 2012). "Potential diagnostic value of P16 expression in premalignant and malignant cervical lesions.". J Res Med Sci 17 (5): 428-33. PMID 23626605.
- ↑ Hu, WW.; Tao, JH.; Li, GM.; Xu, X.; Yang, XM. (Mar 2010). "[Value of ER, VIM, CEA and p16 detection in the diagnosis and differential diagnosis of primary endocervical and endometrial adenocarcinomas].". Nan Fang Yi Ke Da Xue Xue Bao 30 (3): 526-8, 531. PMID 20335127.