Difference between revisions of "Uterine tubes"
| (13 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
[[Image:Normal Fallopian Tube, Human (2760475010).jpg|thumb|Cross section of a Fallopian tube with decidualization. [[H&E stain]]. (WC/euthman)]] | |||
'''Uterine tubes''', also known as the '''Fallopian tubes''', serve as a connection between the [[ovary|ovaries]] and the [[uterus]]. It is where fertilization usually takes place. | '''Uterine tubes''', also known as the '''Fallopian tubes''', serve as a connection between the [[ovary|ovaries]] and the [[uterus]]. It is where fertilization usually takes place. | ||
| Line 14: | Line 15: | ||
#*Nucleus more luminal. | #*Nucleus more luminal. | ||
#**Nuclei stick-out like a golf tee. | #**Nuclei stick-out like a golf tee. | ||
#Secretory cells. | #Secretory cells. (???) | ||
#*Basal cells, fried egg-like. | #*Basal cells, fried egg-like. | ||
Images: | See also: | ||
*[[Walthard cell rest]]. | |||
===Images=== | |||
www: | |||
*[http://faculty.une.edu/com/abell/histo/ampovidw.jpg Fallopian tube (une.edu)].<ref>URL: [http://faculty.une.edu/com/abell/histo/histolab3f.htm http://faculty.une.edu/com/abell/histo/histolab3f.htm]. Accessed on: 18 October 2011.</ref> | *[http://faculty.une.edu/com/abell/histo/ampovidw.jpg Fallopian tube (une.edu)].<ref>URL: [http://faculty.une.edu/com/abell/histo/histolab3f.htm http://faculty.une.edu/com/abell/histo/histolab3f.htm]. Accessed on: 18 October 2011.</ref> | ||
*[http://medpics.ucsd.edu/index.cfm?curpage=image&course=hist&mode=browse&lesson=37&img=669 Fallopian tube (medpics.ucsd.edu)]. | *[http://medpics.ucsd.edu/index.cfm?curpage=image&course=hist&mode=browse&lesson=37&img=669 Fallopian tube (medpics.ucsd.edu)]. | ||
| Line 42: | Line 47: | ||
{{Main|Ditzels}} | {{Main|Ditzels}} | ||
==Paratubal cyst== | ==Paratubal cyst== | ||
*Also known as ''Hydatid cyst of Morgagni'' and ''Hydatid of Morgagni''. | |||
===General=== | ===General=== | ||
*Very common. | *Very common. | ||
*May lead to ovarian torsion if very large.<ref name=pmid22840942>{{Cite journal | last1 = Thakore | first1 = SS. | last2 = Chun | first2 = MJ. | last3 = Fitzpatrick | first3 = K. | title = Recurrent ovarian torsion due to paratubal cysts in an adolescent female. | journal = J Pediatr Adolesc Gynecol | volume = 25 | issue = 4 | pages = e85-7 | month = Aug | year = 2012 | doi = 10.1016/j.jpag.2011.10.012 | PMID = 22840942 }} | *May lead to ovarian torsion if very large.<ref name=pmid22840942>{{Cite journal | last1 = Thakore | first1 = SS. | last2 = Chun | first2 = MJ. | last3 = Fitzpatrick | first3 = K. | title = Recurrent ovarian torsion due to paratubal cysts in an adolescent female. | journal = J Pediatr Adolesc Gynecol | volume = 25 | issue = 4 | pages = e85-7 | month = Aug | year = 2012 | doi = 10.1016/j.jpag.2011.10.012 | PMID = 22840942 }} | ||
</ref> | </ref> | ||
*Associated with [[obesity]].<ref>{{Cite journal | last1 = Muolokwu | first1 = E. | last2 = Sanchez | first2 = J. | last3 = Bercaw | first3 = JL. | last4 = Sangi-Haghpeykar | first4 = H. | last5 = Banszek | first5 = T. | last6 = Brandt | first6 = ML. | last7 = Dietrich | first7 = JE. | title = Paratubal cysts, obesity, and hyperandrogenism. | journal = J Pediatr Surg | volume = 46 | issue = 11 | pages = 2164-7 | month = Nov | year = 2011 | doi = 10.1016/j.jpedsurg.2011.07.011 | PMID = 22075351 }}</ref> | |||
===Gross=== | ===Gross=== | ||
| Line 82: | Line 89: | ||
===Sign out=== | ===Sign out=== | ||
====Left then right==== | ====Left then right==== | ||
<pre> | |||
A. Fallopian Tube, Left, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
B. Fallopian Tube, Right, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
</pre> | |||
<pre> | <pre> | ||
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | ||
| Line 99: | Line 114: | ||
====Right then left==== | ====Right then left==== | ||
<pre> | |||
A. Fallopian Tube, Right, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
B. Fallopian Tube, Left, Tubal Ligation: | |||
- Fallopian tube within normal limits, consistent with complete cross sections. | |||
</pre> | |||
<pre> | <pre> | ||
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: | ||
| Line 113: | Line 136: | ||
B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: | ||
- FALLOPIAN TUBE WITHIN NORMAL LIMITS. | - FALLOPIAN TUBE WITHIN NORMAL LIMITS. | ||
</pre> | |||
====Both in one container==== | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation: | |||
- Pieces of Fallopian tube within normal limits, consistent with | |||
complete cross sections. | |||
</pre> | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Partial Excision: | |||
- Pieces of Fallopian tube within normal limits, consistent with | |||
complete cross sections and fibril ends. | |||
</pre> | |||
=====Incomplete cross sections at microscopy===== | |||
<pre> | |||
Submitted as "Right and Left Fallopian Tubes", Tubal Ligation: | |||
- Fallopian tubes within normal limits, incomplete cross sections | |||
seen at microscopy; clinical correlation is suggested. | |||
</pre> | |||
=====Mild inflammation===== | |||
<pre> | |||
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation: | |||
- Pieces of Fallopian tube with mild inflammation otherwise within | |||
normal limits, consistent with complete cross sections. | |||
</pre> | </pre> | ||
| Line 120: | Line 170: | ||
- FALLOPIAN TUBE WITH PARATUBAL CYSTS AND FOCAL FIBROSIS. | - FALLOPIAN TUBE WITH PARATUBAL CYSTS AND FOCAL FIBROSIS. | ||
- OVARY WITHIN NORMAL LIMITS. | - OVARY WITHIN NORMAL LIMITS. | ||
</pre> | |||
====Tubes with fimbria==== | |||
<pre> | |||
Submitted as "Right and Left Fallopian Tube Segments", Excision: | |||
- Fallopian tubes with fimbria within normal limits; complete cross sections seen. | |||
</pre> | </pre> | ||
| Line 138: | Line 194: | ||
*+/-Clusters of neutrophils = abscess; known as ''suppurative salpingitis''. | *+/-Clusters of neutrophils = abscess; known as ''suppurative salpingitis''. | ||
Images | ====Images==== | ||
<gallery> | |||
File:Salpingitis_-_low_mag.jpg | Salpingitis - low mag. (WC) | |||
File:Salpingitis_-_high_mag.jpg | Salpingitis - high mag. (WC) | |||
File:Granulomatous_salpingitis_-_intermed_mag.jpg | Granulomatous salpingitis - intermed mag. (WC) | |||
File:Granulomatous_salpingitis_-_high_mag.jpg | Granulomatous salpingitis - high mag. (WC) | |||
</gallery> | |||
===Stains=== | ===Stains=== | ||
If organisms are seen on routine stains: | If organisms are seen on routine stains: | ||
| Line 152: | Line 209: | ||
*[[GMS stain]] +ve/-ve. | *[[GMS stain]] +ve/-ve. | ||
*[[PASD stain]] +ve/-ve. | *[[PASD stain]] +ve/-ve. | ||
==Ectopic pregnancy== | |||
{{Main|Ectopic pregnancy}} | |||
==Adenofibroma== | ==Adenofibroma== | ||
| Line 211: | Line 271: | ||
*[[AKA]] ''tubal intraepithelial carcinoma''. | *[[AKA]] ''tubal intraepithelial carcinoma''. | ||
{{Main|Serous tubal intraepithelial carcinoma}} | {{Main|Serous tubal intraepithelial carcinoma}} | ||
==Serous carcinoma of the fallopian tube== | |||
{{Main|Serous carcinoma of the fallopian tube}} | |||
=See also= | =See also= | ||
Latest revision as of 05:11, 4 November 2024
.jpg)
Uterine tubes, also known as the Fallopian tubes, serve as a connection between the ovaries and the uterus. It is where fertilization usually takes place.
This was ignored in the past... current thinking is that it may be the real culprit in what is often labeled as "ovarian cancer".[1]
Normal uterine tube
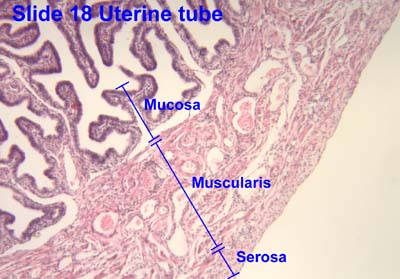
Architecture:
- Finger-like projections into the lumen.
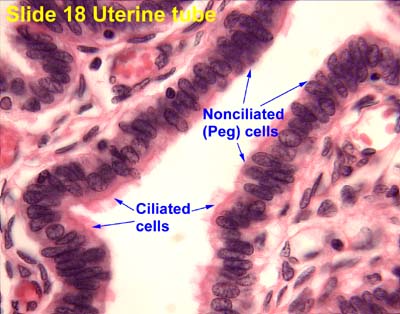
Cells:
- Ciliated cell.
- Columnar.
- Eosinophilic cytoplasm.
- Non-ciliated cell (AKA Peg cell).
- Nucleus more luminal.
- Nuclei stick-out like a golf tee.
- Nucleus more luminal.
- Secretory cells. (???)
- Basal cells, fried egg-like.
See also:
Images
www:
- Fallopian tube (une.edu).[2]
- Fallopian tube (medpics.ucsd.edu).
- Uterine tube - cells (ouhsc.edu).
- Uterine tube - wall (ouhsc.edu).
Overview
Benign lesions
Benign neoplasm
Pre-malignant
Malignant diagnoses
- Serous carcinoma.
- Endometrioid adenocarcinoma.[3]
Ditzels
Paratubal cyst
- Also known as Hydatid cyst of Morgagni and Hydatid of Morgagni.
General
Gross
- Thin walled-cyst with serous fluid.
Microscopic
Features:
- Simple cyst with ciliated (tubal) epithelium.
Sign out
PARATUBAL CYST, RIGHT, EXCISION: - BENIGN SIMPLE CYST.
No epithelium
PARATUBAL CYST, LEFT, EXCISION: - BENIGN FIBROUS TISSUE COMPATIBLE WITH CYST WALL.
Tubal ligation
- Abbreviated TL.
General
- Done to control fertility.
Microscopic
See normal uterine tube.
DDx:
- Salpingitis - inflammatory cells.
- Serous carcinoma - nuclear atypia (marked), nuclear pleomorphism, prominent nucleoli.
- Tubal intraepithelial carcinoma - discrete papillary growth, loss of nuclear polarity, nuclear atypia.
- Endometriosis.
Sign out
Left then right
A. Fallopian Tube, Left, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections. B. Fallopian Tube, Right, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections.
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS.
A. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS. B. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS.
Right then left
A. Fallopian Tube, Right, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections. B. Fallopian Tube, Left, Tubal Ligation: - Fallopian tube within normal limits, consistent with complete cross sections.
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS. B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS, CONSISTENT WITH COMPLETE CROSS SECTIONS.
A. FALLOPIAN TUBE, RIGHT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS. B. FALLOPIAN TUBE, LEFT, TUBAL LIGATION: - FALLOPIAN TUBE WITHIN NORMAL LIMITS.
Both in one container
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation:
- Pieces of Fallopian tube within normal limits, consistent with
complete cross sections.
Submitted as "Fallopian Tubes Right and Left", Partial Excision:
- Pieces of Fallopian tube within normal limits, consistent with
complete cross sections and fibril ends.
Incomplete cross sections at microscopy
Submitted as "Right and Left Fallopian Tubes", Tubal Ligation:
- Fallopian tubes within normal limits, incomplete cross sections
seen at microscopy; clinical correlation is suggested.
Mild inflammation
Submitted as "Fallopian Tubes Right and Left", Tubal Ligation:
- Pieces of Fallopian tube with mild inflammation otherwise within
normal limits, consistent with complete cross sections.
Surgical resection of previous tubal ligation
LEFT FALLOPIAN TUBE AND OVARY, LEFT SALPINGO-OOPHORECTOMY: - FALLOPIAN TUBE WITH PARATUBAL CYSTS AND FOCAL FIBROSIS. - OVARY WITHIN NORMAL LIMITS.
Tubes with fimbria
Submitted as "Right and Left Fallopian Tube Segments", Excision:
- Fallopian tubes with fimbria within normal limits; complete cross sections seen.
Specific diagnoses
Salpingitis
- Also suppurative salpingitis.
- Also granulomatous salpingitis.
General
- Benign.
- May be part of pelvic inflammatory disease.
Microscopic
Features:
- Inflammatory cells:
- Neutrophils = acute.
- Lymphocytes and plasma cells = chronic.
- +/-Granulomas; known as granulomatous salpingitis.
- +/-Clusters of neutrophils = abscess; known as suppurative salpingitis.
Images

Salpingitis - low mag. (WC)

Salpingitis - high mag. (WC)

Granulomatous salpingitis - intermed mag. (WC)

Granulomatous salpingitis - high mag. (WC)




{kind=link}
{kind=link}
{kind=link}
Stains
If organisms are seen on routine stains:
- Gram stain +ve/-ve.
Granulomatous inflammation:
- Ziehl-Neelsen stain +ve/-ve.
- GMS stain +ve/-ve.
- PASD stain +ve/-ve.
Ectopic pregnancy
Adenofibroma
General
- Rare.[6]
- More frequently seen than in the past -- presumably as pathologists are looking more closely at the Fallopian tube.
- Cannot be disguished from ovarian adenofibroma.[6]
Gross
- Solid, nodular.
Microscopic
Features:[6]
- Stroma + glandular elements.
- Glandular elements: secretory cells and ciliated cells.
IHC
Features:
- Stroma:[6]
- CD10 +ve.
- Inhibin +ve.
Salpingitis isthmica nodosa
General
- Associated with infertility and ectopic pregnancy.[9]
- SIN is uncommonly bilateral.[10]
Diagnosis (clinical):
- Hysterosalpingography.[11]
- Finding: diverticula.
Notes:
- The male cousin of this is: vasitis nodosa.
Microscopic
Features:[12]
- Nodular thickening of the tunica muscularis of the isthmic portion.
- Cystically dilated glands.
- +/-Complete obliteration of tubal lumen.
Images:
{kind=link}
Adenomatoid tumour
See: Adenomatoid tumours (uterine tumours).
General
- Relatively common tumour of the fallopian tube.[13]
Microscopic
See: Adenomatoid tumours (uterine tumours).
Serous tubal intraepithelial carcinoma
Serous carcinoma of the fallopian tube
See also
References
- ↑ Hirst, JE.; Gard, GB.; McIllroy, K.; Nevell, D.; Field, M. (Jul 2009). "High rates of occult fallopian tube cancer diagnosed at prophylactic bilateral salpingo-oophorectomy.". Int J Gynecol Cancer 19 (5): 826-9. doi:10.1111/IGC.0b013e3181a1b5dc. PMID 19574767.
- ↑ URL: http://faculty.une.edu/com/abell/histo/histolab3f.htm. Accessed on: 18 October 2011.
- ↑ Navani, SS.; Alvarado-Cabrero, I.; Young, RH.; Scully, RE. (Dec 1996). "Endometrioid carcinoma of the fallopian tube: a clinicopathologic analysis of 26 cases.". Gynecol Oncol 63 (3): 371-8. doi:10.1006/gyno.1996.0338. PMID 8946874.
- ↑ Thakore, SS.; Chun, MJ.; Fitzpatrick, K. (Aug 2012). "Recurrent ovarian torsion due to paratubal cysts in an adolescent female.". J Pediatr Adolesc Gynecol 25 (4): e85-7. doi:10.1016/j.jpag.2011.10.012. PMID 22840942.
- ↑ Muolokwu, E.; Sanchez, J.; Bercaw, JL.; Sangi-Haghpeykar, H.; Banszek, T.; Brandt, ML.; Dietrich, JE. (Nov 2011). "Paratubal cysts, obesity, and hyperandrogenism.". J Pediatr Surg 46 (11): 2164-7. doi:10.1016/j.jpedsurg.2011.07.011. PMID 22075351.
- ↑ 6.0 6.1 6.2 6.3 Bossuyt, V.; Medeiros, F.; Drapkin, R.; Folkins, AK.; Crum, CP.; Nucci, MR. (Jul 2008). "Adenofibroma of the fimbria: a common entity that is indistinguishable from ovarian adenofibroma.". Int J Gynecol Pathol 27 (3): 390-7. doi:10.1097/PGP.0b013e3181639a82. PMID 18580316.
- ↑ Stedman's Medical Dictionary. 27th Ed. Lippincott Williams & Wilkins.
- ↑ URL: http://www.medcyclopaedia.com/library/topics/volume_iv_2/s/salpingitis_isthmica_nodosa.aspx. Accessed on: 28 July 2010.
- ↑ Jenkins, CS.; Williams, SR.; Schmidt, GE. (Oct 1993). "Salpingitis isthmica nodosa: a review of the literature, discussion of clinical significance, and consideration of patient management.". Fertil Steril 60 (4): 599-607. PMID 8405510.
- ↑ Skibsted, L.; Sperling, L.; Hansen, U.; Hertz, J. (Jul 1991). "Salpingitis isthmica nodosa in female infertility and tubal diseases.". Hum Reprod 6 (6): 828-31. PMID 1757522.
- ↑ URL: http://radiology.rsna.org/content/154/3/597.abstract. Accessed on: 28 July 2010.
- ↑ Chawla, N.; Kudesia, S.; Azad, S.; Singhal, M.; Rai, SM.. "Salpingitis isthmica nodosa.". Indian J Pathol Microbiol 52 (3): 434-5. doi:10.4103/0377-4929.55019. PMID 19679986.
- ↑ Christensen C (1990). "Adenomatoid tumors of the uterus". Eur. J. Gynaecol. Oncol. 11 (2): 85–9. PMID 2199199.
- ↑ Visvanathan, K.; Vang, R.; Shaw, P.; Gross, A.; Soslow, R.; Parkash, V.; Shih, IeM.; Kurman, RJ. (Dec 2011). "Diagnosis of serous tubal intraepithelial carcinoma based on morphologic and immunohistochemical features: a reproducibility study.". Am J Surg Pathol 35 (12): 1766-75. doi:10.1097/PAS.0b013e31822f58bc. PMID 21989347.