Difference between revisions of "Inflammatory skin disorders"
(→Lichen planus: +stains) |
m (→Stains) |
||
| Line 215: | Line 215: | ||
===Stains=== | ===Stains=== | ||
*PAS-D or PAS-F to | *PAS-D or PAS-F to exclude a fungal infection. | ||
===Sign out=== | ===Sign out=== | ||
Revision as of 07:25, 5 July 2013
Inflammatory skin disorders, also inflammatory skin diseases, are a significant part of dermatopathology. They lead to trepidation among pathologists that don't see lots of skin. Non-inflammatory skin disease is covered in dermatologic neoplasms and non-malignant skin disease.
Classification
- Bullous.
- Interface.
- Nodular & diffuse.
- Spongiotic.
- Vasculitis.
- Perivascular.
- Panniculitis.
- Psoriasiform.
Tabular comparison of inflammatory skin disease (adapted from Brinster[1][2]):
| Pattern | Key histologic feature | Subclassifications | Example | Image |
| Bullous | large "empty spaces" | -subcorneal -suprabasillar -subepidermal |
-pemphigus foliaceus -pemphigus vulgaris -dermatitis herpetiformis |
(WC) |
| Interface | inflammation at DE junction | -vacuolar (minimal) -lichenoid (band-like) |
-erythema multiforme, SLE -lichen planus |
|
| Nodular & diffuse | intradermal inflammatory infiltrate - nodular and/or diffuse | -neutrophic -lymphocytic -plasmic -eosinophilic -histocytic |
-follicular occlusion triad, ruptured cyst/follicle -CTCL, reactive -plasma cell neoplasm, syphilis -eosinophilic cellulitis, Kimura disease -granuloma annulare, sarcoidosis, TB |
(WC) |
| Spongiotic | small empty spaces between keratinocytes - can see squamous bridges (best seen at high power); +/- quasi-microvacuolar appearance | -acute -subacute -chronic |
-poison ivy -nummular dermatitis -atopic dermatitis |
severe (WC), mild (WC) |
| Vasculitis | inflammation of vessel wall/vessel was destruction | -small vessel -medium vessel -large vessel |
-leukocytoclastic vasculitis -PAN -giant cell arteritis |
(WC) |
| Perivascular | inflammation around vessels | -neutrophilic -lymphocytic -mastocytic -eosinophilic |
-cellulitis -viral exanthem, Rx reaction -mastocytosis -insect bite, Rx reaction |
(WC) |
| Panniculitis | inflammation of adipose tissue | -septal -lobular |
-erythema nodosum, scleroderma panniculitis -erythema induratum, infection |
|
| Psoriasiform | epidermal thickening and long rete ridges |
-regular -irregular |
-psoriasis -lichen simplex chronicus |
(WC) |
Notes:
- DE junction = dermal-epidermal junction.
- The "empty space" in bullous disease in situ is filled with fluid.
Non-specific patterns
Psoriasiform pattern
General
- Can be subclassified.
DDx:
- Psoriasis vulgaris (most common).
- Psoriatic arthritis.
- Drug-induced.
- Dermatomycosis (fungal infection).
- Others.
Microscopic
- Regular epidermal thickening - as very long rete ridges (described as "test tube-morphology") - key feature.
- Epidermis between rete ridges thin ("thinning of suprapapillary plate").
- Parakeratosis.
- Thin/absent granular layer.
- Dilated blood vessels in superficial dermis.
- Neutrophil clusters (Munro microabscess).
Specific diseases
Seborrheic dermatitis
General
- Very common.
Microscopic
Features:[4]
- Spongiosis (epidermal edema).
- Acanthosis (epidermal thickening).
- "Follicular lipping" = parakeratosis with neutrophils.
- Perivascular neutrophils and lymphocytes.
Lupus erythematosus
General
- A group of skin diseases - includes:
- The systemic disease, systemic lupus erythematosus, that typically has multi-organ involvement.
Microscopic
Features - classic:
- Lymphocytic interface dermatitis.[5]
- Basal layer vacuolization.[6]
- Intradermal mucin.
- Thin epidermis.
- Compact stratum corneum.
DDx:
- Discoid lupus erythematosus.
- Drug reaction (drug-induced lupus erythematosus).
- Solar elastosis - may be confused with mucin; vacuolar interface dermatitis not present
Images:
- WC:
Discoid lupus erythematosus
General
- Typically self-limited and isolated.
- It is not associated with systemic lupus erythematosus.
Microscopic
Features:[7]
- Lymphocytic interface dermatitis with basal layer vacuolation and keratinocyte apoptosis.
- Deep dermal lymphocytes.
- Basket weave stratum corneum.
- Dermal mucin.
- Thick dermal-epidermal basement membrane.
DDx:
Image:
Dermatomyositis
- For the muscle manifestations see: Neuromuscular_pathology#Dermatomyositis.
General
- Complement mediated disease - membrane attack complex.
- Usually middle age.
- Associated skin rash is common.
- May precede or follow muscle pathology.
- Associated with malignancy in approximately 10% of cases.[8]
Clinical:
- Jo-1 +ve.
Gross
- Have lesions on the knuckles - Gottron's papules.
Microsopic
Features:
- Vacuolar interface dermatitis (lymphocytic inflammation at the dermal-epidermal junction).
- +/-Loss of rete ridges.
DDx:
- Lupus.
Lichen planus
- Should not be confused with lichen planus-like keratosis.
- Abbreviated LP.
General
- An oral pathology - classically.
- May be seen where the sun don't shine - penis,[9] vulva and vagina.[10]
Etiology:
- Autoimmune disease, T-cell–mediated.[11]
Clinical:[12]
- 6 Ps: pruritic (itchy), purple, polygonal, planar papules and plaques.
Note:
- Clinically, lichen planus and lichen sclerosus are similar. The main difference is lichen planus involves mucous membranes.[13]
Gross
- Wickham striae = white lines/dots.
- Due to hypergranulosis.
Microscopic
- Loss of basal cells (stratum basale) -- key feature.
- Loss of rete ridges/formation of pointed rete ridges "sawtoothing".
- Interface dermatitis (lymphocytes at dermal-epidermal junction).
- Hypergranulosis; stratum granulosum thickened (grossly seen as "Wickham stria" = white lines).
- Hyperkeratosis; stratum corneum thickened.
- Necrotic basal cell in dermis = colloid bodies = Civatte bodies.[16]
- Pink bodies approximately the size of a keratinocyte.
Notes:
- Hyperkeratosis and hypergranulosis are not seen in erythema multiforme.
- Colloid bodies = cytoid bodies = Civatte bodies = hyaline bodies = apoptotic bodies.[17]
DDx:
- Bullous disease, subepithelial vesicular.
- Lichenoid keratosis (lichen planus-like keratosis) - parakeratosis prominent, no oral mucosal involvement.
- Fungal infection.[18]
Images
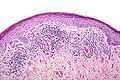
Lichen planus - intermed. mag. (WC/Nephron)
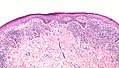
Lichen planus - low mag. (WC/Nephron)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stains
- PAS-D or PAS-F to exclude a fungal infection.
Sign out
FORESKIN, CIRCUMCISION: - LICHEN PLANUS.
VULVA, LEFT POSTERIOR FORCHETTE, BIOPSY: - LICHEN PLANUS.
Micro
The sections show skin with a lymphoplasmacytic interface dermatitis, basal cell loss, hypergranulosis, hyperkeratosis, and loss of the rete ridges.
Lichen sclerosus
Microscopic
Features:[19]
- Subepithelial fibrosis - key feature.
Psoriasis
General
- Chronic skin condition +/- systemic involvement:[20]
- Arthritis, i.e. psoriatic arthritis.
- Myopathy.
- Enteropathy, e.g. inflammatory bowel disease.
- Syondylitic joint disease (spondylos = vertebrae[21]).
- Other considerations:
- Drug-induced psoriasis.[22]
Clinical
- Auspitz sign = pin-point bleeding on removal of scale.
- Koebner phenomenon = lesions form at site of trauma.
Common locations:[20]
- Knees, elbows, scalp, glands penis.
Microscopic
Features:[20]
- Acanthosis + long rete ridges (psoriasiform hyperplasia).
- Parakeratosis.
- Dilated vessels in superficial dermis (give rise to Auspitz sign).
- Spongiform pustules = PMNs in stratum spinosum.
- PMNs in parakeratotic stratum corneum (Munro microabscess).
- Thinning of the suprapapillary plate.
- The epidermis between rete ridges is thinner than in the normal adjacent skin - key feature.
DDx:
- Dermatomycosis (fungal infection).
- Drug reaction.
Note:
- Dermatophytosis = ring worm; dermatophystosis != dermatomycosis.
Stains
- PASD stain -ve for fungal organisms.
Lichen striatus
General
Features:[23]
- Benign, self-limited.
Clinical:
- Linear rash usu. on lower extremity.
- Associated with atopy, lichen sclerosus.[23]
- Children.
Clinical image:
Microscopic
Features:
- "Ball and glove" pattern:
- Rete ridges (glove) surround nexts of lymphocytes (ball).
- Hyperkeratosis.
- Parakeratosis.
DDx:
Images:
Lichen aureus
General
- Rare.
Clinical:[24]
- Plaques + minimal scale - erythematous/golden.
Microscopic
Features:[24]
- Lymphocyte-predominant perivascular pattern.
- May have features suggestive of vacuolar interface pattern.
- Fibrosis of superficial papillary dermis.
Images:
Granuloma faciale
General
- Considered a vasculitis.[25]
Microscopic
Features:[26]
- Neutrophilic vasculitis - often subtle:
- Neutrophils within blood vessel walls.
- Vessels destruction (fibrinoid necrosis or nuclear dust).
- Mixed inflammatory superficial dermal infiltrate.
- Eosinophils, neutrophils, plasma cells, histiocytes.
- Lesion separated from the (normal) epidermis (Grenz zone).[25]
DDx of chronic fibrosing leukocytoclastic vasculitis:[26]
- Granuloma faciale.
- Erythema elevatum diutinum - lacks Grenz zone.
- Inflammatory pseudotumour.
Image:
Atopic dermatitis
General
- Very common - especially in children.[27]
- Most children outgrow the condition.
Microscopic
Features:
- Spongiotic dermatitis.
DDx:
Images:
{kind=link}
Sweet syndrome
General
- Uncommon.
Microscopic
Features:
- Nodular and diffuse pattern - neutrophils predominant - without pus.
DDx rips:
- Rheumatoid neutrophilic dermatitis.
- Bowel-associated dermatosis-arthritis syndrome.
- Pyoderma gangrenosum.
- Sweet syndrome.
Image:
{kind=link}
Granuloma inguinale
- Not to be confused with granuloma annulare.
- Previously known as donovanosis.
General
- Infection caused by Klebsiella granulomatis - Gram-negative, rod-shaped bacteria.
- Used to be known as Calymmatobacterium granulomatis.[29]
Location:
Clinical:[30]
- Sexually transmitted.
- Nodule or papule developing into a painless ulcer in the inguinal region.
- No lymphadenopathy (unlike syphilis).
Microscopic
Features:
- Donovan bodies - key feature:
- Rod-shaped bodies within histiocytes.
DDx:
Image:
Stains
- Giemsa stain - highlights organisms.
Pyoderma gangrenosum
General
Clinical
Gross
- Skin ulceration - classically on the legs.[31]
Microscopic
Features:[31]
- Early: lymphocytes cells only in the dermis - often perivascular & vascular.
- +/-Fibrinoid necrosis of vessels at edge of lesion.
- Late: abscess formation (neutrophils).
DDx:
Image:
Necrobiotic xanthogranuloma
- Abbreviated NXG.
General
- Usually elderly.[33]
Gross
Features:
- Periorbital - classic location.[34]
Microscopic
Features:[33]
- "Necrobiotic granuloma":
- Palisading granuloma with a core collagen-like material.
- +/-Cholesterol clefts - common.
- +/-Touton giant cells.
- +/-Atypical foreign body-type giant cells +/- asteroid bodies.
DDx:
- Granuloma annulare.
- Necrobiosis lipoidica - has plasma cells.
- Granuloma-forming infections - positive stains for microorganisms.
Image:
{kind=link}
DDx for pattern
Spongiotic dermatitides
DDx:[1]
- Atopic dermatitis.
- Contact dermatitis.
- Stasis dermatitis.
- Seborrheic dermatitis.
- Nummular dermatitis.
- Spongiotic drug eruption.
Psoriasiform dermatitides
Regular psoriasiform dermatitis
DDx:[1]
- Psoriasis vulgaris.
- Dermatophyte infection.
- Pityriasis rubra pilaris.
Irregular psoriasiform dermatitis
Interface dermatitides
Vacuolar interface dermatitides
DDx:[1]
- Erythema multiforme.
- Lichen sclerosus.
- Fixed drug eruption.
Others:[1]
- Graft versus host disease.
- Dermatomyositis.
- Systemic lupus erythematosus.
- Morbillifrom viral exanthem.
Additional:[35]
- Phototoxic dermatitis.
- Acute radiation dermatitis.
- Erythema multiforme-like drug eruption.
- Lichen sclerosis et atrophicus.
- Erythema dyschromicum perstans (ashy dermatosis).
Super lame mnemonic Danny G & SLE:
- Dermatomyositis, GVHD, SLE, Lichen sclerosus, Erythema multiforme.
Lichenoid interface dermatitides
DDx:[1]
- Lichen planus
- Mycosis fungoides.
- Discoid lupus erythematosus.
- Lichenoid drug eruption.
- Fixed drug eruption.
Additional:[35]
- Lichen planus-like keratosis.
- Lichenoid actinic keratosis.
- Lichen nitidus.
- Pigmented purpuric dermatosis.
- Lichen amyloidosis.
- Pityriasis lichenoides chronica.
- HIV dermatitis.
- Syphilis.
- Urticaria pigmentosa.
- Chronic graft versus host disease.
Bullous disease
Subcorneal bullous disorders
DDx with acantholysis:[1]
DDx without acantholysis:DDx:[1]
- Subcorneal pustular dermatosis (Sneddon-Wilkinson disease).
- Pustular psoriasis.
- Pustular drug eruption (acute generalized exanthematous pustulosis).
Suprabasilar bullous disorders
DDx:[1]
- Pemphigus vulgaris.
- Hailey-Hailey disease (benign familial pemphigus).
- Darier disease.
- Grover disease (transient acantholytic dermatosis).
Memory device - PhD + Grover = Pemphigus vulgaris, Hailey-Hailey, Darier, Grover.
Subepidermal bullous disorders
DDx:[1]
- Bullous pemphigoid.
- Cicatricial pemphigoid.
- Porphyria cutanea tarda.
- Epidermolysis bullosa acquista.
- Dermatitis herpetiformis.
- Linear IgA disease.
Others:
- Insect bite.
- Coma blister.
- Bullous systemic lupus erythematosus.
Mnemonic DELPHI:
- Dermatitis herpetiformis.
- Epidermolysis bullosa acquisita.
- Bullous lupus erythematosis.
- Pemphigoid, bullous.
- Herpes gestationis - rare autoimmune bullous dermatosis of pregnancy, not related to HSV.[36]
- Linear IgA disease.
Dermatitides with perivascular inflammation
Lymphocytes
Lymphocytes (tightly cuffed):[1]
- Infections.
- Medications.
- Malignancy.
- Vitiligo (with absent melanocytes).
- Scleroderma/morphea.
Lymphocytes & plasma cells +/-eosinophils:
- Erythema chronicum migrans (Lyme disease).
Lymphocytes (not tightly cuffed):
- Viral exanthems.
- Drug eruptions.
Lymphocytes & eosinophils:
- Drug reaction.
- Insect bite.
- Dermatophyte infection.
A simple memory device - 6 Ls:[37]
- Lymphoma.
- Pseudolymphoma (cutaneous lymphoid hyperplasia, lymphocytoma cutis).
- Lupus erythematosus.
- Lymphocytic infiltrate of Jessner / tumid lupus erythematosus.
- Polymorphous light eruption.
- Lyme disease.
Neutrophils
DDx:[1]
- Cellulitis.
- Neutrophilic eccrine hidradenitis (idiopathic palmar-plantar hidradenitis)
With eosinophils:
- Urticaria.
Eosinophils
DDx:[1]
- Hypersensitivity reaction/drug reaction.
- Insect bite.
- Bullous pemphigoid, urticarial.
Mast cells
Vasculitis
General DDx:
- Infection.
- Autoimmune.
- Malignancy.
- Toxic (medications).
Small vessel:
Medium vessel:
Medium vessels often with small vessel involvement:
- Churg-Strauss syndrome.
- Microscopic polyangiitis.
- Mixed cryoglobulinemia.
- Connective tissue diseases.
Large vessel:
Nodular and diffuse dermatitides
Neutrophils
With pus (suppurative)
Neutrophils only:
- Follicular occlusion triad.
- Ruptured cyst/follicle.
Neutrophils and eosinophils:
- Halogenoderma.
- Blastomycosis-like pyoderma (pyoderma vegetans) - due to bacterial infection, usu. S. aureus.
Without pus
With vasculitis:
- Neutrophils only: see vasculitides.
- Mixed infiltrate: granuloma faciale, erythema elevatinum diutinum.
Without vasculitis:
- Sweet syndrome.
- Pyoderma gangrenosum.
- Rheumatoid neutrophilic dermatitis.
- Bowel-associated dermatosis-arthritis syndrome.
Lymphocytes
- Reactive lymphoid hyperplasia - may be due to drugs.
- Lymphoid malignancy.
Plasma cells
- Inflammation.
- Plasma cell neoplasms.
- Infections:
- Syphilis - lichenoid/psoriasiform pattern.
- Chancroid.
- Granuloma inguinale.
- Lymphogranuloma venereum.
Eosinophils
- Eosinophilic cellulitis (Wells syndrome).
- Insect bites.
- Hypereosinophilic syndrome (HES).
- Angiolymphoid hyperplasia with eosinophilia (ALHE).
- Kimura disease.
Histiocytes
Granulomatous
Sarcoidal
- Sarcoidosis - have few lymphoid cells around them; thus called "naked granulomas".[2]
Tuberculoid
- Tuberculosis.
- Tertiary syphilis - usu. abundant plasma cells.
- Cutaneous leishmaniasis.
Foreign body-type granulomas
Palisaded granumolas
Blue granuloma:
- Granuloma annulare.
- Wegener granulomatosis.
- Rheumatoid vasculitis.
Red granuloma:
See also
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 Brinster NK (March 2008). "Dermatopathology for the surgical pathologist: a pattern based approach to the diagnosis of inflammatory skin disorders (part I)". Adv Anat Pathol 15 (2): 76–96. doi:10.1097/PAP.0b013e3181664e8d. PMID 18418089.
- ↑ 2.0 2.1 Brinster, NK. (Nov 2008). "Dermatopathology for the surgical pathologist: a pattern-based approach to the diagnosis of inflammatory skin disorders (part II).". Adv Anat Pathol 15 (6): 350-69. doi:10.1097/PAP.0b013e31818b1ac6. PMID 18948765.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1191. ISBN 978-1416031215.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1191. ISBN 978-1416031215.
- ↑ JAH. 20 February 2009.
- ↑ Crowson AN, Magro CM, Mihm MC (April 2008). "Interface dermatitis". Arch. Pathol. Lab. Med. 132 (4): 652–66. PMID 18384217. http://www.archivesofpathology.org/doi/full/10.1043/1543-2165%282008%29132%5B652%3AID%5D2.0.CO%3B2.
- ↑ URL: http://www.dermpedia.org/baby-dermpedia-for-beginners/discoid-lupus-erythematosus. Accessed on: 7 March 2012.
- ↑ Chen YJ, Wu CY, Huang YL, Wang CB, Shen JL, Chang YT (2010). "Cancer risks of dermatomyositis and polymyositis: a nationwide cohort study in Taiwan". Arthritis Res. Ther. 12 (2): R70. doi:10.1186/ar2987. PMC 2888225. PMID 20398365. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2888225/.
- ↑ Teichman, JM.; Sea, J.; Thompson, IM.; Elston, DM. (Jan 2010). "Noninfectious penile lesions.". Am Fam Physician 81 (2): 167-74. PMID 20082512.
- ↑ Gupta, R.; Bansal, B.; Singh, S.; Yadav, I.; Gupta, K.; Kudesia, M. (2009). "Lichen planus of uterine cervix - the first report of a novel site of occurrence: a case report.". Cases J 2: 9306. doi:10.1186/1757-1626-2-9306. PMID 20062629.
- ↑ URL: http://emedicine.medscape.com/article/1078327-overview. Accessed on: 11 September 2010.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1191. ISBN 978-1416031215.
- ↑ McPherson, T.; Cooper, S.. "Vulval lichen sclerosus and lichen planus.". Dermatol Ther 23 (5): 523-32. doi:10.1111/j.1529-8019.2010.01355.x. PMID 20868406.
- ↑ URL: http://emedicine.medscape.com/article/1078327-overview. Accessed on: 11 September 2010.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1192. ISBN 978-1416031215.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 604. ISBN 978-1416054542.
- ↑ URL: http://www.careforumwales.org/cell-carcinoma/histopathologic-terminology.html. Accessed on: 28 August 2011.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 36. ISBN 978-0443066542.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1065-6. ISBN 0-7216-0187-1.
- ↑ 20.0 20.1 20.2 Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 603. ISBN 978-1416054542.
- ↑ URL: http://medical-dictionary.thefreedictionary.com/spondylosis. Accessed on: 28 August 2011.
- ↑ Milavec-Puretić, V.; Mance, M.; Ceović, R.; Lipozenčić, J. (Mar 2011). "Drug induced psoriasis.". Acta Dermatovenerol Croat 19 (1): 39-42. PMID 21489366.
- ↑ 23.0 23.1 Taniguchi Abagge, K.; Parolin Marinoni, L.; Giraldi, S.; Carvalho, VO.; de Oliveira Santini, C.; Favre, H.. "Lichen striatus: description of 89 cases in children.". Pediatr Dermatol 21 (4): 440-3. doi:10.1111/j.0736-8046.2004.21403.x. PMID 15283785.
- ↑ 24.0 24.1 Hazan, C.; Fangman, B.; Cohen, D. (2007). "Lichen aureus.". Dermatol Online J 13 (1): 23. PMID 17511956.
- ↑ 25.0 25.1 URL: http://dermatlas.med.jhmi.edu/derm/indexDisplay.cfm?ImageID=1289066309. Accessed on: 23 September 2011.
- ↑ 26.0 26.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 198-9. ISBN 978-0443066542.
- ↑ URL: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001856/. Accessed on: 28 December 2011.
- ↑ URL: http://dermatology.cdlib.org/94/NYU/Apr2002/7.html. Accessed on: 4 January 2012.
- ↑ O'Farrell N (December 2002). "Donovanosis". Sex Transm Infect 78 (6): 452–7. PMC 1758360. PMID 12473810. http://sti.bmj.com/cgi/pmidlookup?view=long&pmid=12473810.
- ↑ Bezerra, SM.; Jardim, MM.; Silva, VB. (Jun 2011). "Granuloma inguinale (Donovanosis).". An Bras Dermatol 86 (3): 585-6. PMID 21738983.
- ↑ 31.0 31.1 31.2 Brooklyn, T.; Dunnill, G.; Probert, C. (Jul 2006). "Diagnosis and treatment of pyoderma gangrenosum.". BMJ 333 (7560): 181-4. doi:10.1136/bmj.333.7560.181. PMC 1513476. PMID 16858047. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1513476/.
- ↑ Wong, WW.; Machado, GR.; Hill, ME.. "Pyoderma gangrenosum: the great pretender and a challenging diagnosis.". J Cutan Med Surg 15 (6): 322-8. PMID 22202507.
- ↑ 33.0 33.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 629. ISBN 978-0443066542.
- ↑ Fernández-Herrera, J.; Pedraz, J. (Jun 2007). "Necrobiotic xanthogranuloma.". Semin Cutan Med Surg 26 (2): 108-13. doi:10.1016/j.sder.2007.02.008. PMID 17544963.
- ↑ 35.0 35.1 Alsaad, KO.; Ghazarian, D. (Dec 2005). "My approach to superficial inflammatory dermatoses.". J Clin Pathol 58 (12): 1233-41. doi:10.1136/jcp.2005.027151. PMC 1770784. PMID 16311340. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770784/.
- ↑ URL: http://emedicine.medscape.com/article/1063499-overview. Accessed on: 23 September 2011.
- ↑ URL: http://www.dermpathmd.com/mnemonics/mnemonics_dermatopathology.htm. Accessed on: 23 September 2011.